 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
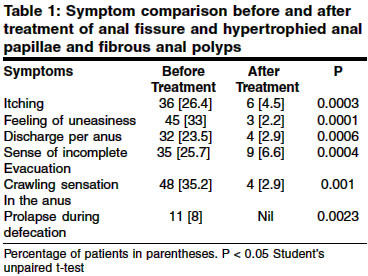
Indian Journal of Surgery, Vol. 66, No. 3, June, 2004, pp. 164-168 Original Article Removal of hypertrophied anal papillae and fibrous polyps improves outcome of anal fissure surgery Gupta Pravin J Consulting Proctologist, Gupta Nursing Home, D/9, Laxminagar, Nagpur-440022 Code Number: is04040 ABSTRACT BACKGROUND: The presence of Hypertrophied anal papillae and fibrous anal polyps are often ignored in the proctology practice. But the experience is that they tend to produce minor but disturbing symptoms. This study is aimed to assay the impact and utility of attending to these two conditions concurrently while dealing with cases of fissure in ano. MATERIAL AND METHODS: A study was carried out in 136 patients of chronic anal fissure having concomitant hypertrophied anal papillae or fibrous anal polyp. After relieving sphincter spasm by sphincterotomy, the polyps or papillae were destroyed using the radio frequency device. A comparison was made for the associated complaints like pruritus, pricking sensation, wetness, crawling in the anus etc. before and after removal of the papillae or polyps by an independent observer blinded to the procedure. RESULTS: After one month of the procedure, the associated symptoms were reduced to a significant amount along with a near total decline in the primary complaints of pain and bleeding. There was significant reduction in pruritus (P=0.0003), discharge per anus (P=0.0006), crawling sensation in the anus (P=0.0004) and sense of incomplete evacuation (P=0.001) At the follow up after 18 months, only 9% patients had recurrence of either anal fissure or symptoms like pruritus. CONCLUSION: This study establishes that removal of hypertrophied anal papillae and fibrous polyps should be carried out as a routine during surgical treatment of anal fissure. This would add to effectiveness and completeness of the procedure.INTRODUCTION Anal papillae,[1] which are also called as anal fibroma, papillitis hypertrophicans, or "cat tooth", are the fine points of projections of the extreme upper end of anal canal skin at the mucocutaneous junction. Small Papillae remain usually asymptomatic. An elongated anal papilla associated with pain and/or bleeding at defecation is sometimes encountered in infancy. Hemorrhage into a hypertrophied anal papilla can cause sudden rectal pain. A prolapsed papilla may become nipped by contraction of the sphincter mechanism after defecation.[2] Occasionally, a red edematous papilla is encountered with local pain and a purulent discharge from the associated crypt. This condition2 is called as ′papillitis′ with `cryptitis.′ The enlargement of the existing anal papillae is a consequence of a chronic inflammatory process and fibrotic proliferation within the range of the Linea dentata, the ano rectal zone and the distal rectal mucosa. The hypertrophied anal papillae are prone to undergo considerable fibrous thickening to acquire a rounded expanded tip, which is then known as a fibrous polyp.[3] Occasionally the occurrence of hypertrophied anal papillae is reported after operational interferences in the anal region. Dilated vein, white area and a large hypertrophied anal papilla are often found in prolapsing types of hemorrhoids.[4] In the literature, the prevalence of these papillae varies between 6% and 60% of all anoscopically-examined patients.[5] They are equally found in both the sexes. The anal papillae, if get hypertrophied or are converted into anal polyps, can produce a foreign body feeling and discharge from the anus. Subsequently, a toxic irritative anal eczema may develop. Histologically, the papillae consists of an edematous, loosened up, fibrotic connective tissue in parts, with increase in capillary contents. Occasionally akanthosis and widened disk epithelium may be seen, but they never proceed to malignant degeneration.[6] The papillae and polyps should be differentiated from subanodermal anal venous thrombosis, condyloma, and rectal adenoma.[7] Patients with fibrous polyp complain of projection of something inexplicable from the anus. A case of giant hypertrophied anal papilla complicated by massive anal bleeding and prolapse is reported.[8] The objective of this study was to demonstrate that hypertrophied anal papillae and fibrous anal polyps are responsible for minor but disturbing complaints on the part of the patient and hence should necessarily be attended to and be removed during surgical treatment of anal fissure and further that they can conveniently be removed by the radio frequency surgical device. MATERIAL AND METHODS This non-randomized study was conducted at Fine Morning Hospital and Gupta Nursing Home, Nagpur, India, between July 1999 and December 2000.In all, 136 patients of chronic fissures in ano with hypertrophied anal papillae and/or fibrous polyp were studied. All the patients under study had hypertrophied anal papillae. The numbers of papillae were ranging from 2 to 4 [mean of 3.2]. The papillae, which felt on digital examination, were considered ′large′. Papillae, which were not palpable and were visible only on anoscopy, were termed ′small′ papillae. In 17 of the studied patients, anal polyp was found in association. 16 of these patients had a single polyp while in one patient, there were two. Out of these, 11 patients had polyps of prolapsing type, which used to project out during defecation and getting reduced spontaneously after the act. The remaining 6 were of non-prolapsing type. Exclusion criteria An informed consent was obtained from all the patients. No special pre operative preparation was carried out. The study was approved by the local ethics committee and was carried out according to the declaration of Helsinki. All of the patients received a dose of laxative [Lactulose 20ml] on the night before the procedure. Radio frequency surgery for the hypertrophied anal papillae and fibrous anal polyps. Few surgeons practice removal of the papillae or polyps by snipping them with scissors or shaving them with scalpel or electrocautry after being crushed.[9] We, instead, have used the radio frequency technique to effectively destroy these papillae and polyps. Radio frequency surgery is a method of simultaneous cutting and coagulating of the tissues.10 We used a dual radio frequency generator 4 MHz from Ellman International, Hewlett, N.Y. for this procedure. An interchangeable ball electrode for coagulation and a round loop electrode for shaving the desired tissue were extensively used in the procedure. Procedure The commonest sites where the papillae were seen were at 3, 7 and 11′O clock position with the patient in a lithotomy position. The next common sites were at 1, 5 and 9′O clock. The base of large papillae and fibrous polyp were circumferentially coagulated by the ball electrode first and then they were excised by the round loop electrode of the radio frequency surgical unit. Minor bleeding, when encountered, was coagulated by touching the source with the ball electrode. This additional procedure of removal of papillae or polyps took a mean period of 2 minutes to complete. The patients were given analgesics [Ketoprofen 250 mg twice a day] for a week and were prescribed a stool softener [Lactulose 15 ml at bed time] for a month. All the patients were discharged within 12 hours of the procedure. They were reviewed after 30 days. Comparative study Statistical analysis RESULTS After one month, anoscopy showed total absence of these papillae. The fissures were healed and there was no sphincter spasm. Patients who were treated for fibrous polyps did have some amount of oedema and mild elevation at the site of destruction. 17 patients [12.5%] complained of postoperative bleeding which was minor, streaking the stool and lasted for a maximum period of four days. The comparison of the findings at a follow up after 1 month is given in [Table - 1]. Subsequent follow up after 18 months DISCUSSION Anal papillae are present in almost 50-60% patients examined. Usually, these are small, cause no symptoms, and could be regarded as normal structures.[11] However, if it is a case of hypertrophy and if the papillae start projecting in the anal canal, it requires attention and suitable treatment. In such cases, it may lead to increased mucus leak resulting in increased anal moisture. They are liable to cause trauma during the passage of stool and may become inflamed. In addition, when papilla is converted into a fibrous polyp, it gives rise to symptoms like prolapse, which may require frequent manual repositioning. The polyp is considered as one of the differential diagnosis of rectal prolapse.[12] Symptoms like pruritus,[13] foreign body sensation, pricking, a sense of incomplete evacuation and heaviness in the anal region have also been reported by the patients. As a routine practice, these pathologies are not given any importance.[14] There is very brief account of this entity in the standard textbooks and other references. Secondary goals of fissure surgery sometimes require the removal of hypertrophied papilla and skin tag as well as the removal of inflammatory and fibrotic tissue surrounding the fissure.[15] Customarily, for symptomatic papillae or polyp, its removal by crushing the base, excision after ligation or electrocautrization has been suggested. We have instead, used the radiofrequency device to successfully tackle these pathologies. Radio frequency surgery, not to be confused with electro surgery, diathermy, spark-gap circuitry, or electrocautry, uses a very high frequency radio wave. Unlike electrocautry or diathermy, the electrode releasing radiofrequency waves remains cold. This is possible because of use of very high frequency current of 4 MHz, as compared to 0.5 to 1.5 MHz used in the electrocautry, which produces greatest amount of tissue alteration. In contrast to true cautery, which causes damage similar to 3rd degree burns, the tissue damage that does occur in radio frequency surgery is superficial and is comparable to that which occurs with Lasers. Histologically, it has been shown that tissue damage with radio frequency surgery is much less than that of a conventional scalpel and practically equals the one caused by a cold scalpel.[16] The radio frequency device offers several unique advantages over conventional surgical modalities. It provides for a controlled balance in simultaneously cutting and coagulating through a single instrument.[17] Since it is used in direct contact with tissues, the surgeon gets the tactile feedback and continues to exert the same familiar and confident control over the job as is experienced during the traditional knife technique. The technique has a self-sterilizing effect and leaves behind a bacteria free zone around the place of application. The radiofrequency device allows cutting and coagulation of tissues in an atraumatic manner, contrary to the electric bistoury. The advantages of radiofrequency over electrocautery and laser energy surgery reside in its precision in ablating tissues and in its control of operation. With radiofrequency, the targeted tissue temperatures stay localized within a 60-900C range thus limiting heat dissipation and damage to adjacent tissue. In contrast, electrocautery, diathermy, and laser temperatures are significantly higher (750-9000C) which result in significant heat propagation in excess of the desired therapeutic need. These differences allow for radiofrequency being found more accurate, minimally invasive and less morbid without compromising the treatment efficacy and durability. While techniques using conventional scalpel apparently works in an atraumatic way, the prominence of bleeding from the wound forces the surgeon to coagulate the bleeders with traditional electrocautery or diathermy more frequently than radiofrequency. The radio waves can seal the small blood vessels without creating any char, whereas the cautery or elcetrosurgical instruments create heat at the tip of the instruments to seal the affected portion with transferred heat, and in the process invariably damage the adjacent healthy tissues, which consequently cause more edema and postoperative pain. Anal papillomata tend to produce a discharge resulting in a sodden perianal skin with itching and discomfort. Wallis believed that hypertrophied anal papillae played an important part in the etiology of pruritus ani. A large papilla that projects at the anus might conceivably interfere with proper anal closure and thus predispose to leakage of mucus, which could lead to pruritus. Hypertrophied anal papilla should be included in the differential diagnosis of a smooth mass located near the anal verge, especially in a patient with a history of chronic anal irritation or infection.18 The presence of a fibrous anal polyp is shown to have a statistically significant association with operative treatment.[19] Though we have used the radiofrequency equipment to tackle these pathologies, we do not intend to promote the same. The procedure can also be carried out with sharp excision with scissors or electrocautery. The equipment used by us is significantly more expensive that other methods. We, nevertheless, admit that the associated symptoms found in patients of anal fissure are partly due to the primary disease itself and are partly getting alleviated after the treatment of fissure. A prospective and randomized comparative study between removal and no removal of the papillae and polyps would have been more conclusive of this contention. But after comparing the symptoms before and after removal of the papillae and polyps, it seems that these pathological lesions too were also responsible for the minor but disturbing complaints. Their removal had definite therapeutic benefits,20 which results in improved patient satisfaction. CONCLUSION In our considered opinion, removal of hypertrophied anal papillae and polyps encountered during surgical treatment of chronic fissure in ano would add to effectivity of the procedure, better patient compliance and a sense of job satisfaction. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04040t1.jpg] |
| |||||||||

{kind=link}