 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
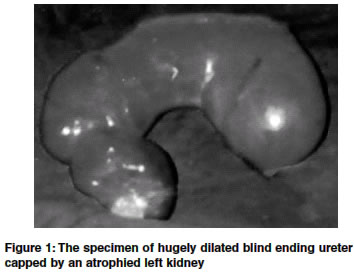
Indian Journal of Surgery, Vol. 66, No. 3, June, 2004, pp. 175-177 Case Report Distal ureteric atresia presenting as an abdominal lump in an adult Bhattacharjee Prosanta Kr , Ghosal Sushil , Sharma GDutta Department of Surgery, R. G. Kar Medical College and Hospital, Kolkata Code Number: is04044 ABSTRACT A 26-year-old female, presented with discomfort and a lump in the left side of abdomen. Examination showed a non-tender cystic mass in the left lumbar region extending down to the pelvis, the lower limit being palpable through the left fornix. Investigations revealed a cystic mass extending from the left renal area to the pelvis and a non-visualized left kidney. Cystoscopy could not identify the left ureteric orifice. Surgical exploration showed a blind ending left ureter as a cystic mass, containing clear fluid capped by a hypoplastic left kidney. The mass extended from the left renal area to the pelvis. Left sided nephroureterectomy was performed.INTRODUCTION Ureteric atresia is a rare congenital abnormality. In distal atresia the ureter fails to communicate with the bladder and terminates close to it as a cul-de-sac. The proximal canalized ureter generally presents as a cystic mass. It may present in the infancy or childhood as an abdominal mass. But because of the relatively greater increase in the size of the abdominal cavity it is less apparent in adults and may remain unnoticed through out life.[1] It may be incidentally discovered as a mass during investigations of persistent fever.[1] One such case of distal ureteric atresia in an adult is reported because of its rarity. CASE REPORT A 26-year-old female, presented with vague discomfort in the left side of the abdomen for 18 months and a lump in the left side of the abdomen noticed for 8 months. Bowel and bladder habits, appetite, menstrual cycle were normal. On examination the patient was thin built, weighing 34kgs, afebrile and slightly pale. There was a non-tender, soft, cystic mass, measuring 5" x 6", extending from the left costal margin down into the pelvis. It was fixed and had a well defined upper margin; the lower margin was not palpable. The mass showed no movement with respiration. The peristaltic sounds were normal. Per rectal examination revealed the lower limit of the cystic mass to lie anteriorly and to the left. Routine examination of blood revealed hemoglobin 10.1 gm% with normal total and differential counts. Blood urea and creatinine were 28mg% and 1.1 mg% respectively. Urinalysis was normal. Plain x-ray of abdomen showed a soft tissue shadow extending along the left flank of the abdomen down towards the pelvis. USG revealed a cystic mass extending from the left lumbar region to the pelvis with improperly delineated left kidney. IVU showed a well functioning, larger than normal right kidney and non- visualized left kidney. Later films of the series showed smooth extrinsic indentation of the dome of the bladder. Isotopic renogram also showed normal perfusion of the tracer on the right and a completely nonfunctioning left kidney.Retrograde pyelography was attempted, however, cystoscopy failed to identify the left ureteric orifice. Patient was explored with the provisional diagnosis of a nonfunctioning hydronephrotic left kidney. Exploration revealed a cystic mass situated retroperitoneally on the left side. Proper mobilization of the left colon revealed it to be hugely dilated left ureter extending from the left renal region down to the pelvis, ending blindly by indenting the dome of the bladder but without communicating with it. Left kidney was small and atrophic [Figure - 1] and the dilated ureter contained large quantity of clear fluid. Opposite kidney and ureter were larger than normal in size due to compensatory hypertrophy but were otherwise normal and no other congenital abnormalities were detectable. Left sided nephroureterectomy was performed. Post operative recovery was uneventful. Histopathology report of the atrophied kidney showed rudimentary glomeruli and tubules suggestive of dysplastic kidney. DISCUSSION It has been observed that in higher vertebrates the development of the kidney and ureter is a complicated multistep process that involves genes like Wilms′ tumour (WT1), c-ret oncogene, Wnt4 and forming.[2] Ureteric atresia results from failure of canalization of a segment of ureter because of ischemic damage to that portion during the process of elongation of the ureteral bud.[3] It may be unilateral or even bilateral and can involve any portion of the ureter.[3] It is commonly associated with ipsilateral or contralateral, renal or ureteric duplication.[1] In distal ureteric atresia the terminal portion of the ureter ends blindly before establishing a communication with the bladder, a point to be remembered while differentiating it from a clinically similar condition of obstructed megaureter. In the latter there is a functional stenosis or narrowing of distal part of the ureter in the presence of ureterovesical communication. Ureteric atresia is difficult to diagnose preoperatively. Conditions with which it is likely to be confused clinically are hydronephrosis, megaureter, retroperitoneal cysts, tumors, and ovarian tumors.[1] Magnetic resonance imaging and laparoscopy, when available, are important aids in preoperative diagnosis.[4],[5] When ureteric atresia presents in the infancy and childhood, the presentation is that of an abdominal mass, due to huge cystic dilatation of the ureter proximal to the atretic segment. It has been reported in a 9 years old child with multicystic dysplasia in half of horseshoe kidney with lower ureteric atresia.[6] On the other hand a blind ending ureter with a noninfected, dysplastic kidney may remain unnoticed through out life.1 It may be accidentally discovered as a mass or during investigation for persistent fever (when the content gets infected).[1] In this reported case, the lean and thin stature of the lady probably brought the cyst to her notice and prompted her to seek medical advice. Though laparoscopy was certainly an important option both for diagnosis and treatment, it could not be used in this patient because of its non-availability at the time of surgery. Since her left kidney was atrophied and nonfunctioning while the opposite kidney was functionally normal a left sided nephroureterectomy was decided upon. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04044f1.jpg] |
| |||||||||

{kind=link}