 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
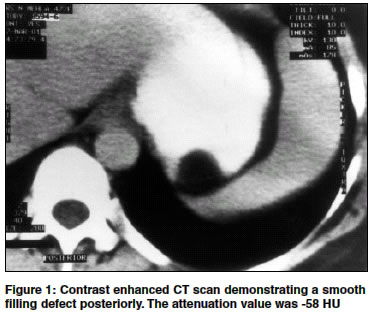
Indian Journal of Surgery, Vol. 66, No. 3, June, 2004, pp. 177-179 Case Report Lipoma of the stomach Singh Rajdeep , Bawa Amarpreet S Department of Surgery, Government Medical College and Hospital, Sector 32, Chandigarh Code Number: is04045 ABSTRACT Lipomas are benign tumours of adipose tissue. They are rare in the stomach, but when present, may produce haematemesis, pain or dyspepsia. A case of gastric lipoma is reported and relevant management options discussed.INTRODUCTION With the widespread use of endoscopy and improvements in radiological techniques, more and more gastric lesions are being picked up. It is often difficult to differentiate benign neoplasms (<2% of all gastric tumours) from low grade sarcomas,[1] and although lipomas form only 3% of benign gastric tumours,[2] they can be the cause of much diagnostic confusion, vis-à-vis, gastric cancer. CASE REPORT A 44 year old female was admitted with history of upper abdominal pain only. General and systemic examination was unremarkable. Except an elevated ESR (39 mm 1st hour-Wintrobe′s method), all laboratory investigations were normal.Ultrasound examination of the abdomen was normal. On fibreoptic endoscopy, a 3 x 3 cm smooth, elevated area with normal overlying mucosa was present along the greater curvature at the fundus. Endoscopic punch biopsy was inconclusive. Contrast enhanced abdominal CT revealed a smooth, rounded, homogeneous, polypoidal lesion along the posterior wall of stomach [Figure - 1]. On laparotomy, a bulge was visible over the posterior aspect of fundus, without any breach of the overlying serosa. Gastrotomy was done here and a 3 x 3 cm soft, smooth submucosal mass was found with normal overlying mucosa. Frozen section examination revealed lipoma, so a wedge resection with 2 cm margin was performed. The post operative period was uneventful. The patient is well one year post surgery. Histopathology confirmed it to be a sub mucosal lipoma of the stomach. DISCUSSION Lipomas are rare in the gastrointestinal tract, where they form 6% of all gastrointestinal tumours.[2] Common sites of involvement are the colon and small bowel; stomach is uncommonly affected. When present, the commonest site of involvement is the antrum (75%), but they can be found in all parts except the cardia and pylorus.[3] They are usually single and submucosal (95%) in position.[3] Although malignant change may occur in lipomas present in other parts of the body, it has never been reported in the stomach. Synchronous gastric cancer and lipomas have been reported, but are probably coincidental.[4] The aetiology of gastric lipoma is unknown. The common view favors embryologically sequestered adipose tissue. However, since they are seen in an older age group only, an acquired aetiology seems more probable.[5] Although early symptoms mimic peptic ulcer disease, gastric lipomas usually present with haemorrhage (53%), abdominal pain (37%), pyloric obstruction (33%) or dyspepsia (26%). Haemorrhage may be chronic or acute and occurs due to pressure necrosis and ulceration of the overlying mucosa.[5] Rarely, cases may present with gastroduodenal intussusception. The typical feature on endoscopy is a sharply defined smooth swelling with intact mucosa. A yellowish appearance and "tenting" of the mucosa when picked up by biopsy forceps is highly suggestive.[4] If the mucosa is pinched off, fat may be seen to protrude out of the opening. When lipomas are pushed, the forceps sink in, giving a characteristic "cushion" like appearance.[4] As conventional biopsy is inconclusive due to submucosal position of the tumour, electrocautery of the mucosa with repeat endoscopic biopsy from the same site after 2 days has been suggested.[6] Endoscopic ultrasound is highly sensitive for submucosal masses but it cannot reliably differentiate between benign and malignant pathology. Submucosal tumours (including lipomas) give a smooth filling defect with a bull′s eye appearance[7] on barium meal study. Rugae are not distorted and peristalsis is normal. Lipoma is strongly suspected if compression produces a change in shape of the mass.[5] Computerised tomography is highly specific for lipomas.[7] They manifest as well circumscribed submucosal masses with a uniform fat density (-30 to -120 HU). Other gastric tumours which contain fat include angiolipoma, liposarcoma and teratoma. Malignant tumours classically show variable tissue density and septae within the mass.[4] Previously, resections were carried out in all patients with a gastric mass on the assumption that it might be malignant.[2] Advances in endoscopy and imaging techniques have now given an option of conservative management in these patients. If asymptomatic, a lipoma that is conclusively diagnosed preoperatively by means of endoscopic biopsy and computed tomography needs no further intervention.[4] Surgery is presently indicated only when malignancy cannot be ruled out or the symptoms are crippling or life threatening. The use of intraoperative frozen section can avoid unnecessary gastric resections. Although excision with simple closure is recommended, gastrotomy with incision of the mucosa and shelling out of the tumour may be resorted to when it is very large or near the cardia, as wedge resection here will destroy the oesophagogastric angle and promote reflux.[4] In emergency situations (massive haematemesis), formal gastric resection is indicated because the diagnosis cannot usually be confirmed. Laparoscopic resection has been recommended for lipomas less than 6 cm in diameter, or those with endoluminal or extraluminal protrusion.[8] Although submucosal tumours can be shelled out endoscopically, a combined laparoscopic and endoscopic approach is recommended because small perforations can go unnoticed if endoscopy is used alone.[8] REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04045f1.jpg] |
| |||||||||

{kind=link}