 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 4, July-August, 2004, pp. 227-231 Original Article Medical hemostasis in experimental liver resection with antifibrinolytic therapy Cihan Alper, Yilmaz Erdal Department of Surgery of the Medical Faculty of Zonguldak
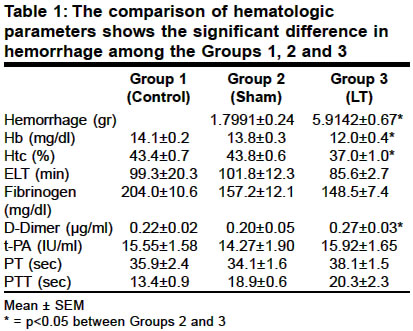
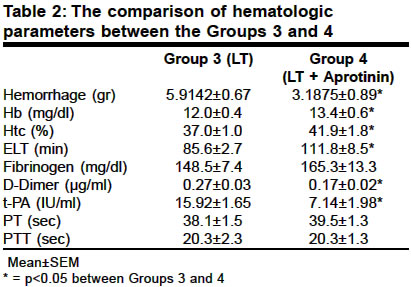
Karaelmas University and Gazi University Code Number: is04053 ABSTRACT AIMS: To study the efficacy of aprotinin in controlling bleeding from parenchymatous organ trauma. MATERIALS AND METHODS: Thirty-two guinea pigs were utilized in 4 groups. While group 1 was control, group 2 was sham operated. Standard liver resection was performed in groups 3 and 4 and aprotinin at dose of 10.000 KIU/kg was infused via jugular catheter ten minutes before the liver resection in group 4. Bleeding amounts were recorded in these groups during 1 hour with weighing the sponges placed into abdomen. Histopathologic, hematologic and fibrinolytic parameters were measured. RESULTS: The amount of bleeding in the liver resection group was 5.9142±0.67 gr whereas it was significantly lower with 3.1875±0.89 gr in the aprotinin administered group (p<0.05). In the aprotinin group the changes in the levels of hemoglobin and hematocrit were also statistically significant (p<0.05). There was no significant difference between the levels of fibrinogen, but there was an increase in euglobulin lysis time (ELT), decrease in tissue plasminogen activator activity and decrease in the level of D-Dimer (p<0.05). CONCLUSIONS: This study demonstrated that aprotinin can decrease the amount of bleeding in parenchymatous organ trauma while suppressing fibrinolytic activity. With aprotinin treatment, there were significant decreases in the levels of D-Dimer, significant reductions in tissue plasminogen activator activity and significant lengthening of the euglobulin lysis time, whereas PT-aPTT levels did not change.KEY WORDS:Medical hemostasis, blood conservation, antifibrinolytic therapy INTRODUCTION In patients undergoing prolonged surgical procedures, in those with trauma[1] and hemorrhage, bleeding resulting from disturbances of coagulation cascade and factor deficiencies has been observed.[2],[3] While dealing with such coagulopathies, the bleeding resulting from the activation of fibrinolytic system should be controlled as well. Non operative management is gaining popularity in haemodynamically stable patients with blunt solid organ injury. Perioperative or postoperative coagulopathies can be caused by the surgical procedure itself, by the pre-existing coagulopathy of the patient, accompanying pathologies, administered medications, hypothermia and dilutional effects. Postoperative hematoma can also cause altered coagulation by increased fibrinolysis.[4] This may be due to the activation of tissue plasminogen, increase of fibrinolysis and secretion of other activators. In patients with rare blood groups, in those with coagulation defects and undergoing surgery and in patients from certain religious groups who refuse to have transfusion, the option of providing perioperative blood preservation is often discussed. For this purpose, several approaches have been described. These are: meticulous surgical hemostasis, utilization of cell saver and ultrafilters and pharmacological hemostasis.[5] However, reduction of bleeding from wounds and there by blood preservation should be the priority. Fibrinolytic system is the conglomerate of mechanisms reacting to fibrin clot while limiting hemostatic reactions. For having destructive effects on fibrin, several substances derived from plasma, platelets, tissues and other blood elements can be used. As an important factor, here we have a serine protease "plasmin" which circulates in the plasma as plasminogen. Several plasminogen activators such as "Tissue Plasminogen Activator (t-PA)" and "Urokinase Plasminogen Activator (u-PA)" play a role in the conversion of plasminogen to plasmin.[6] Aprotinin is a polypeptide isolated from bovine lung, inhibiting serine proteases such as plasmin, trypsin, chymotrypsin and kallikrein.[7],[8] It can provide prevention of uncontrolled activation of the fibrinolytic system or regulation of fibrinolysis. For this purpose, we investigated whether it was medically possible to provide hemostatic balance and decrease the requirement for transfusion in parenchymatous organ damages with experimental liver resection in animals. MATERIALS AND METHODS This study was approved by Gazi University Medical Faculty Experimental Research and Application Ethics Committee. Thirty-two guinea pigs weighing between 450-550 gr were selected as the experimental subjects. They were fed with standard guinea pig feed and food intake was stopped 12 hours prior to the experiment. The study population consisted of four groups each having 8 animals. The temperature of surgical environment during the study was hold at 26-28 C. Ketamin-HCl 50 mg/kg (Ketalar - Eczacýbaþý - Istanbul) and Xylazin-HCl 2 mg/kg (Rompun - Bayer - Turkey, Istanbul) were used for intramuscular anaesthesia. Aprotinin (Protosol - Kamada - Israel) was given intravenous at a dose of 10.000 KIU/kg in ten minutes as antifibrinolytic agent and all surgical interventions were performed in the sterile conditions. The groups were planned as follows; Group 1 (Control): Blood samples were collected and hematologic and biochemical profiles were assessed. Group 2 (Sham): Jugular vein catheterization and laparotomy were performed; dry sponges that have been weighed previously were placed into the abdomen. Sponges were weighed after one hour to evaluate the amount of peritoneal wetting. Blood samples were taken for tests. Group 3 (Liver resection (LR)): Left jugular vein was exposed following anaesthesia, 24G IV cannula (Venflon - Ohmeda, Sweden) was introduced and fixed to the skin with 4/0 silk sutures (Ethicon-UK). The vein was neither transacted nor traumatized. The laparotomies were done from xiphoid to pubis with fixed length and meticulous hemostasis. Intestinal organs were pulled to the left side of the abdomen and left lobe of the liver was taken to the right side of the stomach. Previously weighed dry sponges were placed to the right side of the abdominal cavity. Standard liver resection was made to the anterior border of the liver with semilunar shaped liver knife designed by the authors. Sponges were weighed to evaluate the amount of bleeding every ten minutes during one hour. Fluid replacement was achieved with physiological saline according to the measured volume of the bleeding by weighing these sponges. The sponges were finally weighed to determine the amount of total bleeding at the end of one hour after the hepatic resection. Total abdominal exploration was made to identify any bleeding other than the site of resected liver. Blood samples and liver biopsies were taken for laboratory analysis. Group 4 (LR + Aprotinin): The catheterization of the jugular vein was performed and aprotinin (Portosol - Kamada - Israel) was infused 10.000 KIU/kg in ten minutes via this catheter. After infusion of aprotinin, similar procedures were done as in group 3. Intracardiac blood samples were obtained from all the subjects with 20 ml 16G plastic injectors (FeFarma- Istanbul) after thoracotomy by the same researcher with slow vacuum and single attempt. The blood samples were transferred to the special tubes, and immediately transferred to related laboratories. All blood samples were kept at 4-6oC in ice bags during transfer. The subjects were sacrificed upon obtaining 10-12 ml of blood. Hemoglobin (Hb), hematocrit (Hct) and platelet measurements were performed with "Coulter Counter" (Beckman Coulter, USA). Prothrombin time (PT), partial thromboplastin time (aPTT), fibrinogen and D-Dimer levels were measured with "STA compact" automated coagulometer (Diagnostica Stago Asniers, France) by using specific reagents of the system. ELT was measured with the method described by Love and Prentice.[9] After the clotting time was recorded, the mixture was left to lysis in 37oC incubator and exact lysis time was identified. The results were expressed in minutes."Coaset t-PA (Chromogenix-Sweden) research kit was used for the measurement of tissue plasminogen activator activity (t-PA-act) with manual spectrophotometric technique. The absorbencies of the samples were measured at 405 nm with the spectrophotometer. The difference between sample and blank activities was regarded as the measurement value. The obtained measurements were expressed in IU/ml within a range of 1.5-10 IU/ml according to standard t-PA-act given by the manufacturer. Aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin (TBil) and alkaline phosphatase (ALP) were assayed with Humalyzer-2000 (Human- Germany) spectrophotometer. The complete test kits and specific reagents were utilized and tests were assayed with enzymatic colorimetric spectrophotometer method. For statistical difference each parameter within the groups was compared with Kruskal-Wallis One Way Analysis. In order to identify the subgroups′ responsibility for these differences, comparisons were made with Mann-Whitney U test in pairs. In all the comparisons the level of statistical significance was accepted as p<0.05. RESULTS In the Sham group the sponges placed into the abdomen had an average of 1.7901±0.24 gr increase in their weight after 1 hour due to peritoneal wetting. When bleeding group was compared to sham group, the amount of bleeding was significant with 5.9142±0.67 gr as shown in [Table - 1] (p<0.05). Hb and Hct levels also demonstrated significant decreases. There was a mild decrease in the level of fibrinogen and decrease in ELT that was not of statistical significance. However, the increase in the level of D-Dimer was statistically significant. There was no statistically significant difference in t-PA-acts [Table - 1]. There was no difference between groups 3 and 4 with regards to the PT-PTT levels. In the liver resection group, the amount of bleeding was 5.9142±0.67 gr whereas in the aprotinin administered group it was significantly lower with 3.1875±0.89 gr (p<0.05). In the aprotinin group the changes in the levels of Hb and Hct were also significant (p<0.05). There was no significant difference between the levels of fibrinogen, but there was lengthening of ELT (p<0.05), decrease of t-PA-act (p<0.05) and decrease in the level of D-Dimer (p<0.05). DISCUSSION In the comparison of the control group and the sham group, differences of statistical significance were found between the levels of PTT and fibrinogen. Significant changes in the levels of PTT and fibrinogen while having no change in the level of PT, points out the increase in fibrinolytic activity and the activation of the contact pathway as shown in [Table - 2]. When compared to Group 3, the administration of aprotinin to the study group (Group 4) resulted in a bleeding of 3.1875±-0.89 gr which was significantly lower (p<0.05). Additionally there were significant increases in Hb and Hct values [Table - 1]. With the administration of aprotinin to the study group, fibrinogen levels increased as well; yet, this was not of statistical significance. However, statistically significant increase in ELT, decrease of t-PA level and decrease in the level of D-Dimer, showed the efficacy of aprotinin in preventing the surgical procedure related hyperfibrinolysis. The changes observed in the measurements of D-Dimer, t-PA-act and ELT demonstrates that increased fibrinolytic activity and extrinsic fibrinolytic system pathway were suppressed by aprotinin. The measurement of ELT is an indirect indicator of the concentrations of plasma fibrinogen, plasminogen and plasminogen activators.[9] t-PA-act is one of the direct indicators of the fibrinolytic system. For the evaluation of fibrinolytic system in medical hemostasis, measurement of ELT in addition to t-PA-act has been a controlled approach. Lack of significant differences between the levels of PT and PTT in groups 2, 3 and 4 and increased level of PTT compared to Group 1 not returning to normal with antifibrinolytic treatment decreases the suspicions concerning the possibility of aprotinin causing thrombotic complications. The study conducted by magnetic resonance on a bypass graft after cardiovascular surgery did not reveal an increased risk for the obstruction of the graft.[7],[10] There is a report in 2001 by Molenaar and colleagues about anticoagulant and anti-inflammatory effects of high doses of aprotinin.[11] Young and colleagues also demonstrated the improvement healing of colonic anastomoses with aprotinin via collegenase inhibition.[12] Instead of being treated with medical hemostasis, stress and coagulopathic conditions caused by parenchymatous organ injuries due to blunt traumas may result in unnecessary surgical interventions. In post-operative hematomas and continuous bleedings in the form of leaks, the adverse effects of both the thrombin and the fibrin degradation products and also the decreases in the speed of procoagulant mechanisms due to consumption, results in an increase in coagulopathies.[13] In this study, after a surgical resection, there was an increase in PTT and decrease in fibrinogen, related to subclinical activation of fibrinolytic mechanism. When parenchymatous organ trauma and bleeding were added to the existing situation, despite significant increases in the levels of D-Dimer compared to sham group, there was no change in fibrinogen levels and no significant decrease in ELT demonstrating the fibrinolytic system activation without reaching a pathological dimension. With effective inhibition of kallikrein and plasmin by aprotinin, contact activation of coagulation is inhibited. Contact activation is the stimulator of the intrinsic pathway. This pathway is responsible for the production of thrombin, activation of plasminogen and activation of fibrinolytic system.[14] Aprotinin exerts antifibrinolytic effects by decreasing the formation of fibrin degradation products, activation of á2- antiplasmin and t-PA inhibitor and decreasing the secretion of t-PA from endothelial cells.[15],[16] The concentration of plasma aprotinin should be 250 KIU/ml for the inhibition of kallikrein and 125 KIU/ml for plasmin.[7],[17] All the doses that have been utilized in order to reduce the blood loss and the requirements for homologous blood transfusion have been well tolerated by cardiovascular surgery patients.[7] 10.000 KIU/kg that was used in the study will provide an average concentration of 200 KIU/ml. There were significant differences concerning the amount of bleeding and Hb values between the groups receiving aprotinin at this level and the one not receiving aprotinin, demonstrating the efficacy of antifibrinolytic treatment. With aprotinin treatment, there were significant decreases in D-Dimer levels, in t-PA-act and increase in ELT, whereas PT-PTT values did not change. This shows us that the effect was exerted through the inhibition of fibrinolysis and increase in fibrin stabilization. Local hemostatic materials such as fibrin sealant products[18] and autogenous grafts[19] were investigated to achieve local hemostasis and they were found to be effective in parenchymatous organ hemorrhages. But the local hemostatic applications may be insufficient to control of the hemorrhages due to systemic fibrinolysis. In cases of hyperfibrinolysis resulting from time consuming or major surgical interventions, bleedings due to parenchymatous organ traumas not requiring surgery and other hyperfibrinolytic conditions, medical hemostasis with aprotinin can be safely utilized without causing thrombotic complications. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04053t1.jpg] [is04053t2.jpg] |
| |||||||||

{kind=link}
{kind=link}