
|
Indian Journal of Surgery
Medknow Publications on behalf of Association of Surgeons of India
ISSN: 0972-2068
Vol. 66, Num. 5, 2004, pp. 270-276
|
Indian Journal of Surgery, Vol. 66, No. 5, September-October, 2004, pp. 270-276
Review Article
Choice of digestive tract reconstructive procedure following total gastrectomy: A critical reappraisal
Sharma Dhananjaya
Govt. NSCB Medical College and Allied Hospitals, Jabalpur - 482 003
Correspondence Address:P-10, Medical College Campus, Jabalpur
- 482003, (M.P.) dhanshar@hotmail.com
Code Number: is04070
KEYWORDS: Total gastrectomy, Reconstruction techniques, Out come
assessment
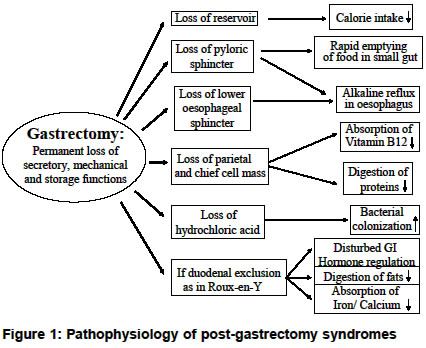
INTRODUCTION Total gastrectomy results in permanent loss of secretory, mechanical and storage functions of the stomach. The altered physiology can be understood from [Figure
- 1]. The rationale behind reconstruction after total gastrectomy is to prevent or minimize these post-gastrectomy disorders. More than 70 types of reconstructive procedures have been tried to minimize post-gastrectomy symptoms. Such a large number suggests that an optimal procedure of reconstruction following total gastrectomy has not been clearly established. This article reviews studies addressing the crucial and contentious issue of gastrointestinal reconstruction following total gastrectomy. PubMed and manual search of published articles were used to search for these studies.
IDEAL RECONSTRUCTION AFTER TOTAL GASTRECTOMY An ideal reconstruction after total gastrectomy should have the following qualities:
- Should ensure that the patient has a sufficiently large enteric reservoir to accommodate normal meals.
- Gradual emptying of reservoir into the small intestine.
- Avoidance of reflux oesophagitis.
- Maintenance of duodenal continuity, if possible.
- Operative procedures should not be time consuming and complicated
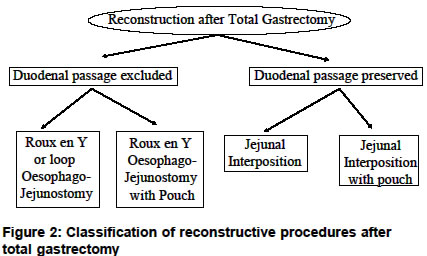
Basically, digestive tract reconstruction following total gastrectomy can be classified into two types according to whether the duodenal tract is excluded or preserved [Figure
- 2]. In principle, pouch procedures for the formation of a neo-stomach were developed to provide a reservoir for food, while the aim behind preservation of the duodenal passage is to restore the anatomy and physiology of the digestive tract. The merits and demerits of these procedures continue to be hotly debated, as results from different studies are contradictory.
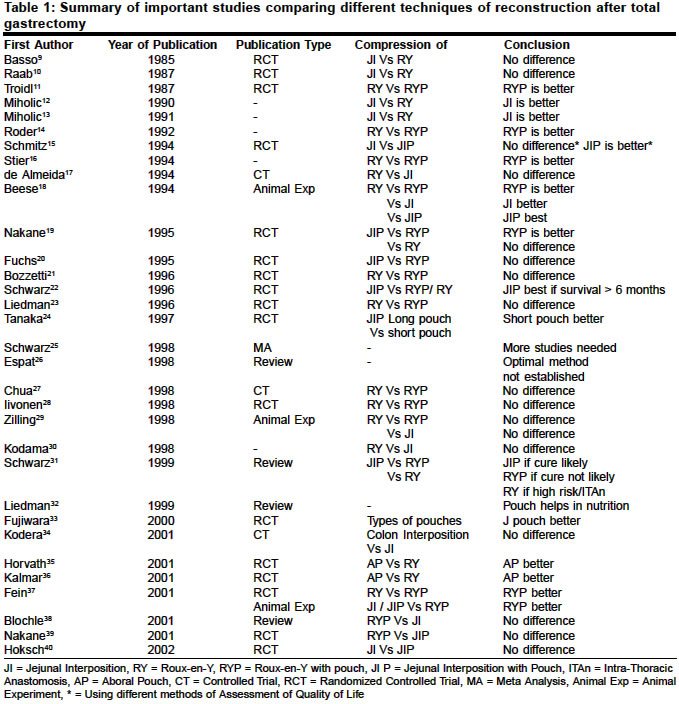
HISTORICAL ASPECT Professor Carl Nicoladonia of Innsbruck, Austria is supposed to have performed the first total gastrectomy in man but no exact reference to this historical incidence can be found.[1] Conner of Cincinnati performed the first recorded total gastrectomy in 1884, but the patient did not survive the surgery. Finally, the credit for performing the first successful total gastrectomy went to Swiss surgeon Schlatter, who restored the gastrointestinal continuity with an end-to-side oesophagojejunostomy in 1897.[2] Gastric resectional surgery, since those days, has come a long way. Better anaesthesia, understanding of asepsis, earlier diagnosis and technical know-how has established total gastrectomy as an accepted and safe procedure. Along with this came the understanding of post-gastrectomy nutritional problems and their impact on the quality of life.[3],[4] This led to various surgical procedures being devised to create a larger reservoir for food, to provide a barrier against intestinoesophageal reflux, and to lengthen the food transit time. Historical evolution of the philosophy of reconstruction following total gastrectomy has been chronicled and should be of interest to the connoisseurs.[3],[5],[6],[7],[8] COMPARISON OF DIFFERENT RECONSTRUCTION METHODS Scientific assessment of post-gastrectomy reconstructed patient is not easy. Anthropometric data, food intake, serum nutritional parameters, haematological survey, small intestinal passage (oral-caecal transit time using lactulose H2 breath test), postprandial symptoms, dumping provocation tests, lipid and carbohydrate absorption, tests for malabsorption and bacterial overgrowth, blood glucose, insulin, cholecystokinin, motilin, secretin, pancreatic polypeptide measurement after stimulation by test meals, body weight and quality of life (QOL) have been used to assess these patients and respective reconstructive methods. QOL includes general and specific physical complaints, satisfaction with life, as well as psychosocial burden. As expected, measurement of QOL has seen the use of varied instruments and scales by different authors; commonly used scales were Visick, Karnofsky, Spitzer′s QOL index, Cuschieri′s assessment, Gastrointestinal Quality of Life Index and EORTC questionnaires. The most remarkable and striking observation after going through the various studies comparing different operative procedures is lack of consensus about which is the best and optimum procedure. Many randomised clinical trials, and experimental studies have been performed comparing different operative procedures and published in the last two decades but have arrived at different conclusions [Table
- 1].[9],[10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23],[24],[25],[26],[27],[28],[29],[30],[31],[32],[33],[34],[35],[36],[37],[38],[39],[40]
EXCLUSION OF DUODENAL PASSAGE
The popularity and preferred usage of this technique could be attributed
to its simplicity as it uses minimum number of anastomoses, diversion
of bile from the oesophagus is an added advantage. However, its critics
mention the altered physiology of duodenal bypass as the main disadvantage
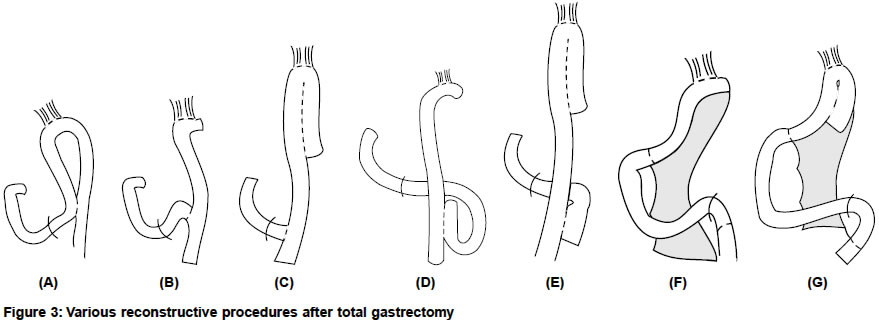
leading to bacterial overgrowth and steatorrhea. The simple loop oesophagojejunostomy
[Figure - 3A] with a distal jejuojejunostomy
achieves the same functional result as a Roux-en-Y oesophagojejunostomy
[Figure - 3B].[41] The
former is, perhaps, safer as its blood supply is less likely to be jeopardized,
but no prospective clinical trial has been performed to compare the two
procedures. The Roux-en-Y procedure when used, has the Roux syndrome
as its other disadvantage due to functional dysmotility of the Roux limb.[42],[43] Fortunately,
dysmotility of the Roux limb is seen in 10-30% cases and severe
forms are even less frequent. Pouch procedures like Hunt-Lawrence pouch
are used with Roux-en-Y procedure [Figure
- 3C] to augment the neogastrium′s
reservoir capacity and to slow down the rapid emptying of food in the
small gut, as both functions are important.[44],[45] It
has been shown that food transit through the pouch follows a linear decreasing
function and is significantly slower compared to the exponential passage
of oesophagojejunostomy, although both patterns remain still significantly
accelerated compared to the physiological ranges of gastric emptying.[16],[46],[47] One
must realize that some altered motility occurs after a Hunt-Lawrence
pouch reconstruction even in asymptomatic patients, which may assume
pathological proportions in symptomatic patients.[48] When the Roux-en-Y pouch procedures were compared with simple Roux-en-Y oesophagojejunostomy, most studies found that patients with pouch reconstruction fared better but significant benefit was not demonstrated in some studies [Table
- 1]. However, research workers have recently realized that beneficial effects of pouch become apparent after a considerable period of time and a real assessment of its benefit must be done after a long follow-up.[40],[49],[50] Now pouch formation is being recommended for patients with severe post-gastrectomy symptoms, with no other plausible explanation than non-existent or insufficient gastric reservoir function, in the hope that they may benefit from re-reconstruction with a jejunal pouch.[51]
It must be emphasized that the pouch formation adds more suture lines, time and complexities to an already major operation and chances of leakage are, at least, theoretically increased.[27] A randomized controlled trial has shown that a short pouch is more effective than a long pouch in maintaining nutrition and in preventing reflux symptoms.[24],[52] Encouraged by the good outcome after Roux-en-Y pouch procedure several modifications of the Hunt-Lawrence pouch were introduced; notable among these are Lygidakis′s modification,[7] aboral
pouch (15-cm long side to side antiperistaltic pouch at the Y anastomosis
of Roux-en-Y, [Figure - 3D][35],[36],[53] or
a double pouch (one at the site of oesophagojejunostomy and another at
the site of Y anastomosis of Roux-en-Y, [Figure
- 3E].[54]
PRESERVATION OF THE DUODENAL PASSAGE Interposition of the
jejunal loop between the oesophagus and the duodenum restores the duodenal
continuity, which maximizes absorption and helps in restoring nutrition.
Another obvious advantage is endoscopic accessibility of the duodenum
and the bilio-pancreatic system. This procedure was first reported by
Henley and later by Longmire [Figure
- 3F].[55],[56] Although
Poth published the first use of jejunal interposed pouch, credit for
popularising the jejunal pouch interposition goes to Cuschieri [Figure
- 3G].[41],[57] There is no doubt that interposition procedures are technically more demanding and complex than those using exclusion of the duodenal passage. Although preservation of the duodenal passage is the more physiological approach to the restoration of the continuity of the digestive tract, surprisingly, the expected impact of the duodenal passage on symptoms, nutrition and outcome could not be ascertained by most of the studies; thereby negating the additional operative effort of jejunum interposition [Table
- 1]. Two randomized control trials have compared the outcome after jejunal interposition and after jejunal interposition with pouch formation; statistically proven benefits for pouch reconstruction could not be demonstrated by either study [Table
- 1]. Perhaps, the reason for failure of the physiological superiority of the preservation of the duodenal passage not getting translated into clinical benefit lies in denervation of the jejunal interposition. This has given rise to using enervated jejunal loop for reconstruction.[58],[59] Similarly, pylorus, pyloric branch of the vagus nerve and lower oesophageal sphincter are being saved in modified surgical procedures ("nearly total gastrectomy" or "function-preserving gastrectomy"), wherever oncologically feasible, in an attempt to improve motility of the reconstructed digestive tract.[60],[61],[62],[63],[64]
USE OF COLON FOR GASTRIC REPLACEMENT Use of colon for gastric replacement, as an operative procedure is not new.[65],[66] A segment of left colon has been used and an attempt has been made to recreate Angle of ′His′ to prevent reflux with satisfactory results.[67] But the use of a segment of transverse colon as a gastric substitute after total gastrectomy failed to show any advantage over those treated by the jejunal interposition.[34] Recently, ileocolon has been used as an intestinal reservoir combined with an anti-reflux mechanism (caecum as reservoir and the ileocecal valve as substitute for pyloric sphincter). The technique seems to reduce the occurrence of postoperative reflux and dumping symptoms.[68],[69] HAND-SEWN OR STAPLED ANASTOMOSES? Randomized controlled trials have shown that operating time, incidence of anastomotic leakage and stenosis, morbidity and hospital stay did not differ significantly between the groups of patients undergoing hand-sewn and mechanically stapled oesophagojejunostomy anastomoses.[70],[71] However, over the years staplers have become quite popular leading to several studies publishing technical refinements for performing oesophagojejunostomy anastomoses and pouch constructions.[27],[43],[72],[73],[74],[75],[76],[77] IS IT WORTHWHILE SAVING PART OF STOMACH I. E. AS IN PARTIAL GASTRECTOMY? Clinicians now realize that malnutrition is not an inevitable consequence of total gastrectomy and can be prevented by an adequate calorie intake, as a close relationship between dietary intake and postoperative nutritional parameters has been observed. In gastrectomized patients a strict nutritional follow-up can ensure an adequate dietary intake.[78] With few exceptions, most authors agree that maintenance of nutritional status and quality of life is similar after partial/ subtotal and total gastrectomy, hence total gastrectomy, when clinically indicated, can be safely done without excessive concern about postoperative nutrition.[79],[80],[81] A randomized controlled trial has shown that patients who undergo subtotal gastrectomy have a better outcome during the first postoperative year, but patients given a gastric substitute after gastrectomy improve with the passage of time and have an even better outcome in the long run.[82] WHICH RECONSTRUCTIVE PROCEDURE SHOULD BE USED? It is not easy to form an opinion on this subject as a review of the literature gives conflicting and confusing guidance [Table
- 1]. There are a few ′bird′s eye view′ reviews and an occasional meta-analysis which shed some light on this vexing question but an optimal procedure for all clinical situations has not been clearly established. However, one conclusion can be drawn: the choice of the procedure to be adopted depends on the key issue of chances of curability of the gastrectomy.[25] This rules out most of the patients being operated in India and other developing countries from being reconstructed with elaborate, complex, time-consuming techniques as late diagnoses of carcinoma stomach is the norm rather than the exception. Logic dictates that in high-risk patients (on account of the shorter operating time) or if the patient is not likely to survive even 6 months, the least demanding procedure of all i.e. Roux-en-Y-reconstruction without pouch should be done. Another indication for Roux-en-Y-reconstruction without pouch is carcinoma of the cardia with intrathoracic anastomosis.[31] But, in all other cases, reconstruction must be performed according to Roux-en-Y with Hunt-Lawrence pouch, as recently acquired knowledge suggests significant benefit of a pouch in the long run.[40],[49],[50]
After total gastrectomy, curatively operated patients might benefit from a jejunal interposition (but there is no hard evidence for the advantage of a pouch) with maintenance of the duodenal passage, as the extra effort and risk of extra anastomoses/suture lines will be worthwhile only in a scenario of assured curative intention. It must be realized that aggressive surgery (extent of lymph node dissection and neighbouring organ resection) for advanced gastric cancer increases the risk of oesophagojejunal anastomotic leakage.[83] For this reason, most Japanese surgeons prefer to reserve jejunal interposition for younger better risk patients, benign disease, and in selected cases of curative resection of carcinoma stomach, especially if the tumour is within or shallower than muscularis propria.[30] REFERENCES
| 1. | Herrington JL. Historical aspects of gastric surgery. In Scott WH & Sawyers JL, editors. Surgery of Stomach duodenum and small intestine. Oxford: Blackwell Scientific Publication; 1992;1-28. Back to cited text no. 1 |
| 2. | Wangensteen OH, Wangensteen SD, Dennis C. The history of gastric surgery. In Westell C, Nyhus LM, Donahue PE, editors. Surgery of the esophagus, stomach and small intestine. Boston: Little Brown and Company; 1994;354-85. Back to cited text no. 2 |
| 3. | Huguier M, Lancret JM, Bernard PF, Baschet C, Le Henand F. Functional results of different reconstructive procedures after total gastrectomy. Br J Surg 1976;63:704-8. Back to cited text no. 3 |
| 4. | Shrock TR, Way LW. Total gastrectomy. Am J Surg 1978;135:348-55. Back to cited text no. 4 |
| 5. | Poth EJ, Smith LB. Gastric pouches: Their evaluation. Am J Surg 1966;112:721-27. Back to cited text no. 5 |
| 6. | Herrington JI. Various types of pouch replacement following total gastrectomy: Historical data and current thoughts regarding total gastrectomy. Am Surg 1968;34:879-87. Back to cited text no. 6 |
| 7. | Lygidakis NJ. Total gastrectomy for gastric carcinoma: A retrospective study of different procedures and assessment of a new technique of gastric reconstruction. Br J Surg 1981;68:649-55. Back to cited text no. 7 |
| 8. | Tittel A, Schumpelick V. History of gastric replacement. Hepatogastroenterology 1989;36:57-62. Back to cited text no. 8 |
| 9. | Basso N, Materia A, Gizzonio D, Marcelli M, De Marco M, Tamburrano G. Nutritional effects of total gastrectomy. A prospective randomized study of Roux-en-Y vs Longmire-Mouchet reconstruction. Ital J Surg Sci 1985;15:335-40. Back to cited text no. 9 |
| 10. | Raab M, van Maercke P, Stutzer H. Quality of life following gastrectomy-a comparison of Longmire and Roux stomach replacement methods. Zentralbl Chir 1987;112:1140-5. (Article in German) Back to cited text no. 10 |
| 11. | Troidl H, Kusche J, Vestweber KH, Eypasch E, Maul U. Pouch versus esophagojejunostomy after total gastrectomy: A randomized clinical trial. World J Surg 1987;11:699-712. Back to cited text no. 11 [PUBMED] |
| 12. | Miholic J, Meyer HJ, Muller MJ, Weimann A, Pichlmayr R. Nutritional consequences of total gastrectomy: The relationship between mode of reconstruction, postprandial symptoms, and body composition. Surgery 1990;108:488-94. Back to cited text no. 12 |
| 13. | Miholic J, Meyer HJ, Balks J, Kotzerke J. Effect of reconstruction method on nutritional status after gastrectomy. Comparison of Roux-Y esophagojejunostomy and jejunum interposition. Chirurg 1991;62:300-5. (Article in German) Back to cited text no. 13 |
| 14. | Roder JD, Herschbach P, Henrich G, Nagel M, Bottcher K, Siewert JR. The quality of life after total gastrectomy for stomach carcinoma. Esophagojejunal plication with pouch versus esophagojejunostomy without pouch. Dtsch Med Wochenschr 1992;117:241-7. (Article in German) Back to cited text no. 14 |
| 15. | Schmitz R, Moser KH, Treckmann J. Quality of life after prograde jejunum interposition with and without pouch. A prospective study of stomach cancer patients on the reservoir as a reconstruction principle after total gastrectomy. Chirurg 1994;65:326-32. (Article in German) Back to cited text no. 15 |
| 16. | Stier A, Holscher AH, Schwaiger M, Siewert JR. Jejunum pouch after total gastrectomy-clinical and scintigraphic studies of function and quality of life. Zentralbl Chir 1994;119:838-44. (Article in German) Back to cited text no. 16 |
| 17. | de Almeida AC, dos Santos NM, Aldeia FJ. Total gastrectomy for cancer: Is reconstruction or a gastric replacement reservoir essential? World J Surg 1994;18:883-8. Back to cited text no. 17 |
| 18. | Beese G, Fuchs KH, Thiede A. Experimental studies of the value of the pouch after gastrectomy. Zentralbl Chir 1994;119:904-10. (Article in German) Back to cited text no. 18 |
| 19. | Nakane Y, Okumura S, Akehira K, Okamura S, Boku T, Okusa T, et al. Jejunal pouch reconstruction after total gastrectomy for cancer. A randomized controlled trial. Ann Surg 1995;222:27-35. Back to cited text no. 19 |
| 20. | Fuchs KH, Thiede A, Engemann R, Deltz E, Stremme O, Hamelmann H. Reconstruction of the food passage after total gastrectomy: Randomized trial. World J Surg 1995;19:698-705. Back to cited text no. 20 |
| 21. | Bozzetti F, Bonfanti G, Castellani R, Maffioli L, Rubino A, Diazzi G, et al. Comparing reconstruction with Roux-en-Y to a pouch following total gastrectomy. J Am Coll Surg 1996;183:243-8. Back to cited text no. 21 |
| 22. | Schwarz A, Buchler M, Usinger K, Rieger H, Glasbrenner B, Friess H, et al. Importance of the duodenal passage and pouch volume after total gastrectomy and reconstruction with the Ulm pouch: Prospective randomized clinical study. World J Surg 1996;20:60-6. Back to cited text no. 22 |
| 23. | Liedman B, Andersson H, Berglund B, Bosaeus I, Hugosson I, Olbe L, et al. Food intake after gastrectomy for gastric carcinoma: The role of a gastric reservoir. Br J Surg 1996;83:1138-43. Back to cited text no. 23 [PUBMED] |
| 24. | Tanaka T, Fujiwara Y, Nakagawa K, Kusunoki M, Utunomiya J. Reflux esophagitis after total gastrectomy with jejunal pouch reconstruction: Comparison of long and short pouches. Am J Gastroenterol 1997;92:821-4. Back to cited text no. 24 |
| 25. | Schwarz A, Beger HG. Gastric substitute after total gastrectomy-clinical relevance for reconstruction techniques. Langenbecks Arch Surg 1998;383:485-91. Back to cited text no. 25 |
| 26. | Espat NJ, Karpeh M. Reconstruction following total gastrectomy: A review and summary of the randomized prospective clinical trials. Surg Oncol 1998;7:65-9. Back to cited text no. 26 |
| 27. | Chua CL. Total gastrectomy for gastric cancer: The rationale for J-pouch reservoir. J R Coll Surg Edinb 1998;43:169-73. Back to cited text no. 27 |
| 28. | Iivonen MK, Ahola TO, Matikainen MJ. Bacterial overgrowth, intestinal transit, and nutrition after total gastrectomy. Comparison of a jejunal pouch with Roux-en-Y reconstruction in a prospective random study. Scand J Gastroenterol 1998;33:63-70. Back to cited text no. 28 |
| 29. | Zilling T, Hansson L, Willen R, Sternby B. Nutritional state, growth rate, and morphology after total gastrectomy with restoration of duodenal passage or Roux-en-Y oesophagojejunostomy with or without a pouch: An experimental study in pigs. Eur J Surg 1998;164:377-84. Back to cited text no. 29 |
| 30. | Kodama I, Kofuzi K, Yano S, Takeda J, Shirouzi K. Jejunal interposition reconstruction after Total gastrectomy. In Sharma Dhananjaya, editor. Debates in Gastrointestinal Surgery. Jabalpur: Banarsidas Bhanot; 1998;66-9. Back to cited text no. 30 |
| 31. | Schwarz A, Schoenberg MH, Beger HG. Pouch stomach reconstruction after gastrectomy. Z Gastroenterol 1999;37:287-91. (Article in German) Back to cited text no. 31 |
| 32. | Liedman B. Symptoms after total gastrectomy on food intake, body composition, bone metabolism, and quality of life in gastric cancer patients-is reconstruction with a reservoir worthwhile? Nutrition 1999;15:677-82. Back to cited text no. 32 |
| 33. | Fujiwara Y, Kusunoki M, Nakagawa K, Tanaka T, Hatada T, Yamamura T. Evaluation of J-pouch reconstruction after total gastrectomy: Rho-double tract vs. J-pouch double tract. Dig Surg 2000;17:475-81. Back to cited text no. 33 |
| 34. | Kodera Y, Yamamura Y, Kanemitsu Y, Shimizu Y, Hirai T, Yasui K, et al, Kato T. Use of a segment of transverse colon as a gastric substitute after total gastrectomy: An audit of 18 patients. Gastric Cancer 2001;4:60-5. Back to cited text no. 34 |
| 35. | Horvath OP, Kalmar K, Cseke L, Poto L, Zambo K. Nutritional and life-quality consequences of aboral pouch construction after total gastrectomy: A randomized, controlled study. Eur J Surg Oncol 2001;27:558-63. Back to cited text no. 35 |
| 36. | Kalmar K, Cseke L, Zambo K, Horvath OP. Compar ison of quality of life and nutritional parameters after total gastrectomy and a new type of pouch construction with simple Roux-en-Y reconstruction: Preliminary results of a prospective, randomized, controlled study. Dig Dis Sci 2001;46:1791-6. Back to cited text no. 36 |
| 37. | Fein M, Fuchs KH, Beese G, Freys SM, Thiede A. Reconstruction modes following gastrectomy. Results of experimental and clinical controlled trials. Zentralbl Chir 2001;126:17-21. (Article in German) Back to cited text no. 37 |
| 38. | Blochle C, Mann O, Stenger AM, Busch C, Izbicki JR. Gastric substitute following gastrectomy. Zentralbl Chir 2001;126:22-5. (Article in German) Back to cited text no. 38 |
| 39. | Nakane Y, Michiura T, Inoue K, Iiyama H, Okumura S, Yamamichi K, et al. A randomized clinical trial of pouch reconstruction after total gastrectomy for cancer: Which is the better technique, Roux-en-Y or interposition? Hepatogastroenterology 2001;48:903-7. Back to cited text no. 39 |
| 40. | Hoksch B, Ablassmaier B, Zieren J, Muller JM. Quality of life after gastrectomy: Longmire's reconstruction alone compared with additional pouch reconstruction. World J Surg 2002;26:335-41. Back to cited text no. 40 |
| 41. | Cuschieri A. Jejunal pouch reconstruction after total gastrectomy for cancer: Experience in 29 patients. Br J Surg 1990;77:421-4. Back to cited text no. 41 |
| 42. | Mathias JR, Fernandez A, Sninsky CA, Clench MH, Davis RH. Nausea, vomiting, and abdominal pain after Roux-en-Y anastomosis: Motility of the jejunal limb. Gastroenterology 1985;88:101-7. Back to cited text no. 42 |
| 43. | van der Mijle HC, Kleibeuker JH, Limburg AJ, Bleichrodt RP, Beekhuis H, van Schilfgaarde R. Manometric and scintigraphic studies of the relation between motility disturbances in the Roux limb and the Roux-en-Y syndrome. Am J Surg 1993;166:11-7. Back to cited text no. 43 |
| 44. | Hunt CJ. Construction of a food pouch from a segment of jejunum as a substitute for stomach in total gastrectomy. Arch Surg 1952;64:601-08. Back to cited text no. 44 |
| 45. | Lawrence WJ Jr. Reservoir construction after total gastrectomy. Ann Surg 1962;155:191-8. Back to cited text no. 45 |
| 46. | McAleese P, Calvert H, Ferguson WR, Laird J. Evaluation of "gastric" emptying time in the J pouch compared with a standard esophagojejunal anastomosis. World J Surg 1993;17:595-9. Back to cited text no. 46 [PUBMED] |
| 47. | Thomas H, Heimbucher J, Fuchs KH, Freys SM, DeMeester TR, Peters JH, Bremner CG, Thiede A. The mode of Roux-en-Y reconstruction affects motility in the efferent limb. Arch Surg 1996;131:63-6. Back to cited text no. 47 |
| 48. | Heimbucher J, Fuchs KH, Freys SM, Clark GW, Incarbone R, DeMeester TR, et al. Motility in the Hunt-Lawrence pouch after total gastrectomy. Am J Surg 1994;168:622-5. Back to cited text no. 48 |
| 49. | Liedman B, Bosaeus I, Hugosson I, Lundell L. Long-term beneficial effects of a gastric reservoir on weight control after total gastrectomy: A study of potential mechanisms. Br J Surg 1998;85:542-7. Back to cited text no. 49 |
| 50. | Miyoshi K, Fuchimoto S, Ohsaki T, Sakata T, Ohtsuka S, Takakura N. Long-term effects of jejunal pouch added to Roux-en-Y reconstruction after total gastrectomy. Gastric Cancer 2001;4:156-61. Back to cited text no. 50 |
| 51. | Liedman B, Hugosson I, Lundell L. Treatment of devastating postgastrectomy symptoms: The potential role of jejunal pouch reconstruction. Dig Surg 2001;18:218-21. Back to cited text no. 51 |
| 52. | Tanaka T, Kusunoki M, Fujiwara Y, Nakagawa K, Utsunomiya J. Jejunal pouch length influences metabolism after total gastrectomy. Hepatogastroenterology 1997;44:891-6. Back to cited text no. 52 |
| 53. | Nadrowsky L. Is a distal jejunojejunal pouch nutritionally ideal in total gastrectomy? Am J Surg 2003;185:349-53. Back to cited text no. 53 |
| 54. | Gioffre' Florio MA, Bartolotta M, Miceli JC, Giacobbe G, Saitta FP, Paparo MT, Micali B. Simple versus double jejunal pouch for reconstruction after total gastrectomy. Am J Surg 2000;180:24-8. Back to cited text no. 54 |
| 55. | Henley FA. Gastrectomy with replacement. Ann R Coll Surg Engl 1953;13:141-60. Back to cited text no. 55 |
| 56. | Longmire WP, Beal JM. Construction of a substitute gastric reservoir following total gastrectomy. Ann Surg 1954;140:467-72. Back to cited text no. 56 |
| 57. | Poth EJ, Cleveland BR. A functional substitution pouch for the stomach. Arch Surg 1967;83:42-54. Back to cited text no. 57 |
| 58. | Nakane Y, Akehira K, Okumura S, Okamura S, Boku T, Okusa T, et al. Jejunal pouch and interposition reconstruction after total gastrectomy for cancer. Surg Today 1997;27:696-701. Back to cited text no. 58 |
| 59. | Kobayashi I, Ohwada S, Ohya T, Yokomori T, Iesato H, Morishita Y. Jejunal pouch with nerve preservation and interposition after total gastrectomy. Hepatogastroenterology 1998;45:558-62. Back to cited text no. 59 [PUBMED] |
| 60. | Sawai K, Takahashi T, Fujioka T, Minato H, Taniguchi H, Yamaguchi T. Pylorus-preserving gastrectomy with radical lymph node dissection based on anatomical variations of the infrapyloric artery. Am J Surg 1995;170:285-8. Back to cited text no. 60 |
| 61. | Yunfu L, Qinghua Z, Yongjia W. Pylorus and pyloric vagus preserving gastrectomy treating 125 cases of peptic ulcer. Minerva Chir 1998;53:889-93. Back to cited text no. 61 |
| 62. | Zhang D, Shimoyama S, Kaminishi M. Feasibility of pylorus-preserving gastrectomy with a wider scope of lymphadenectomy. Arch Surg 1998;133:993-7. Back to cited text no. 62 [PUBMED] [FULLTEXT] |
| 63. | Ohya T, Ohwada S, Iesato H, Takeyoshi I, Kawashima Y, Ogawa T, et al. Jejunal pouch interposition after pylorus-preserving gastrectomy. J Surg Res 1999;86:177-82. Back to cited text no. 63 |
| 64. | Tomita R, Fujisaki S, Tanjoh K, Fukuzawa M. Operative technique on nearly total gastrectomy reconstructed by interposition of a jejunal J pouch with preservation of vagal nerve, lower esophageal sphincter, and pyloric sphincter for early gastric cancer. World J Surg 2001;25:1524-31. Back to cited text no. 64 [PUBMED] [FULLTEXT] |
| 65. | State D, Barclay T, Kelly WD. Total gastrectomy with utilization of a segment of transverse colon to replace the excised stomach. Ann Surg 1951;134:1035-41. Back to cited text no. 65 |
| 66. | Hunnicutt AJ. Repalcing stomach after total gastrectomy with right ileocolon. Arch Surg 1952;65:1-11. Back to cited text no. 66 |
| 67. | Ohwada S, Ogawa T, Nakamura S, Satoh Y, Takeyoshi I, Iwazaki S, et al. Left colon substitution with His' angle following total gastrectomy. Surgical technique using stapling devices. Dig Surg 1999;16:12-5. Back to cited text no. 67 |
| 68. | Sakamoto T, Fujimaki M, Tazawa K. Ileocolon interposition as a substitute stomach after total or proximal gastrectomy. Ann Surg 1997;226:139-45. Back to cited text no. 68 |
| 69. | Metzger J, Degen LP, Beglinger C, Siegemund M, Studer W, Heberer M, et al. Ileocecal valve as substitute for the missing pyloric sphincter after partial distal gastrectomy. Ann Surg 2002;236:28-36. Back to cited text no. 69 |
| 70. | Seufert RM, Schmidt-Matthiesen A, Beyer A. Total gastrectomy and oesophagojejunostomy-a prospective randomized trial of hand-sutured versus mechanically stapled anastomoses. Br J Surg 1990;77:50-2. Back to cited text no. 70 [PUBMED] |
| 71. | Fujimoto S, Takahashi M, Endoh F, Takai M, Kobayashi K, Kiuchi S, et al. Stapled or manual suturing in esophagojejunostomy after total gastrectomy: A comparison of outcome in 379 patients. Am J Surg 1991;162:256-9. Back to cited text no. 71 |
| 72. | Alexander-Williams J. To facilitate the insertion of the EEA autosuture head into the oesophagus. Br J Surg 1982;69:196. Back to cited text no. 72 [PUBMED] |
| 73. | Chung SCS, Crofts H, Li AKC. Balloon dilataion facilitates stapling of oesophagojejunostomy. Surg Gynecol Obstret 1987;164:85-86. Back to cited text no. 73 |
| 74. | Vauthey JN, Maddern GJ, Gertch PH. A simplified technique of oesophagojejunostomy. Surg Gynecol Obstret 1991;173:499-500. Back to cited text no. 74 |
| 75. | Takeshita K, Saito N, Habu H, Saeki I, Honda T, Tani M, et al. Technical devices in jejunal pouch reconstruction following total gastrectomy, including postoperative results. Hepatogastroenterology 1997;44:588-98. Back to cited text no. 75 |
| 76. | Ikeda M, Ueda T, Shiba T. Reconstruction after total gastrectomy by the interposition of a double jejunal pouch using a double stapling technique. Br J Surg 1998;85:398-402. Back to cited text no. 76 |
| 77. | Fujiwara Y, Kusunoki M, Nakagawa K, Tanaka T, Yamamura T, Utsonomija J, et al. The relationship between stapling doughnuts: characteristics and functional results after total gastrectomy. Hepatogastroenterology 1998;45:1177-82. Back to cited text no. 77 |
| 78. | Braga M, Zuliani W, Foppa L, Di Carlo V, Cristallo M. Food intake and nutritional status after total gastrectomy: Results of a nutritional follow-up. Br J Surg 1988;75:477-80. Back to cited text no. 78 |
| 79. | Bozzetti F, Ravera E, Cozzaglio L, Dossena G, Agradi E, Bonfanti G, et al. Comparison of nutritional status after total or subtotal gastrectomy. Nutrition 1990;6:371-5. Back to cited text no. 79 |
| 80. | Buhl K, Lehnert T, Schlag P, Herfarth C. Reconstruction after gastrectomy and quality of life. World J Surg 1995;19:558-64. Back to cited text no. 80 [PUBMED] |
| 81. | Roder JD, Stein HJ, Eckel F, Herschbach P, Henrich G, Bottcher K, et al. Comparison of the quality of life after subtotal and total gastrectomy for stomach carcinoma. Dtsch Med Wochenschr 1996;121:543-9. (Article in German) Back to cited text no. 81 |
| 82. | Svedlund J, Sullivan M, Liedman B, Lundell L. Long term consequences of gastrectomy for patient's quality of life: The impact of reconstructive techniques. Am J Gastroenterol 1999;94:438-45. Back to cited text no. 82 [PUBMED] [FULLTEXT] |
| 83. | Isozaki H, Okajima K, Ichinona T, Hara H, Fujii K, Nomura E. Risk factors of esophagojejunal anastomotic leakage after total gastrectomy for gastric cancer. Hepatogastroenterology 1997;44:1509-12. Back to cited text no. 83 [PUBMED] |
Copyright 2004 - Indian Journal of Surgery
The following images related to this document are available:
Photo images
[is04070f3.jpg]
[is04070f1.jpg]
[is04070t1.jpg]
[is04070f2.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}