 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 5, September-October, 2004, pp. 277-280 Original Article The effectiveness of adjuvant intraperitoneal hyperthermic chemoperfusion after cytoreductive surgery in locally advanced gastric cancer Erhan Erdem, Haluk Alagol Department of General Surgery, Ankara Oncology Training and Research Hospital Code Number: 04081 ABSTRACT BACKGROUND: Intraperitoneal hyperthermic chemoperfusion (IHCP), which is a locoregional treatment used in peritoneal micrometastases in intra-abdominal tumours was first applied in 1980, and since then it has been used as an adjuvant treatment in locally advanced tumours and as palliation in inoperable tumours, especially in tumours of genital and gastrointestinal system origin.
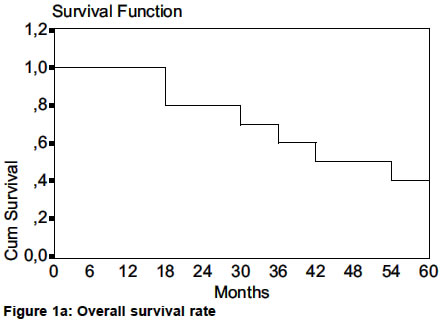
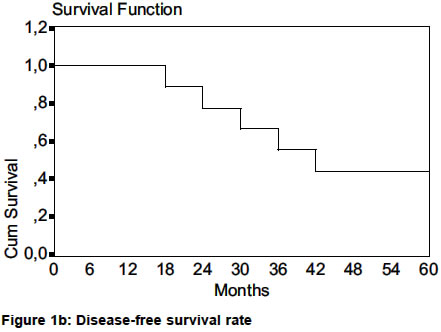
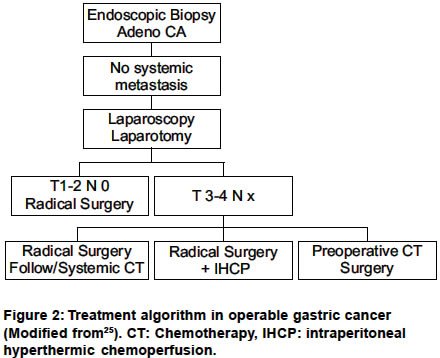
KEY WORDS: Hyperthermic chemoperfusion, gastric cancer INTRODUCTION Hyperthermic perfusion chemotherapy is a locoregional treatment modality that is used as adjuvant treatment in locally advanced operable tumours, and as palliation in inoperable tumours. Thus intraperitoneal hyperthermic chemoperfusion (IHCP) is also a method of locoregional treatment that is used in peritoneal seedings and peritoneal micrometastases in intra-abdominal tumours, especially in the gastrointestinal system and genital tumours. Intraperitoneal administration of chemotherapy has the benefit of higher concentrations of drugs delivered locally to the site of the tumour while diminishing the systemic toxic effects. This method is regarded as the best treatment for the prevention and/or healing of peritoneal seeding from gastrointestinal cancer, especially for gastric cancers, which have a high rate of locoregional recurrence and peritoneal micrometastases.[1],[2],[3] It′s known that in these cases systemic chemotherapy is mostly ineffective.[4],[5],[6] The purpose of this study was to assess the role of IHCP as an adjuvant therapy in locally advanced gastric cancer patients after radical surgery. MATERIALS AND METHODS Ten patients who were diagnosed microscopically as having gastric cancer underwent macroscopic cytoreductive surgery and IHCP between December 1996 and December 2001. The study was approved by the Ethics Committee of the Ankara Oncology Training and Research Hospital (procedures followed in accordance with the standards ethical committee on human experimentation and with the Helsinki Declaration of 1975). Cytoreductive surgery consisted of the removal of all gross tumours and involved organs or peritoneum. So Ro gastric resection was undertaken in all patients with greater and lesser omentectomy, splenectomy and localized peritonectomy (left or right upper quadrant) if there was any involvement or metastasis at peritoneal surface, then D2 lymph node dissection was added. At the end of the operation two drains were inserted in the peritoneal cavity and after the closure of the abdomen, an extra-corporeal circuit conducted IHCP, allow perfusate circulation with at 300-500 ml/min and hyperthermia ranging 40-42°C for 60-90 minutes. The perfusate consisted of 3 L. of saline solution with cytotoxic drugs. We used 10-mg/L mitomycin-C because of its high penetration rate to micronodules and low absorption rate across the peritoneal surface. At the end of the perfusion 1 L. of perfusate was emptied and the rest of it was left in the abdomen for 12 hours. Statistical Analysis The Kaplan-Meier method was used for the calculation of the overall and disease-free survival rates. RESULTS In a total of 10 patients, 5 underwent total and 5 subtotal gastrectomies with omentectomy, splenectomy and D2 lymph node dissection. Localized peritonectomy was also added in 3 of them who had peritoneal involvement. The patients′ tumours were all T3 or T4 and none had organ metastases at the time of surgery. On microscopic examination 1 had musinous and 9 had adenoid cancer and 6 of them had histopathologically proven lymph node metastasis. The patients consisted of 6 women and 4 men with an average age of 59 years (range 25-74). All patients underwent IHCP with mitomycin-C after the surgery. The average hospital stay was 10 days and no systemic and local complications were seen except one atelectasis. The patients were followed-up with regular physical examinations including haematological analysis and tumour markers (CEA, CA 19-9, CA-125) every 3 months, abdominal ultrasonography and upper gastrointestinal endoscopy every 6 months, and abdominal computerized tomography every year. At the end of the first year 2 patients died, one of them from myocardial infarction and she had no evidence of tumour, and the other one from hepatic metastases. In the 24-48 months period 4 other patients also died from liver metastasis and only one of them had peritoneal recurrence. Four patients who completed 5-year survival are still alive and only one of them has a tumour at porta hepatis. Three patients have no complaints, no evidence of tumour or elevation of tumour markers. The 1,2 and 5-year overall and disease-free survival rates were 80, 70, 40% and 90, 60, 30% respectively [Figure - 1a, b]. DISCUSSION The intraperitoneal administration of cytotoxic agents has been used since 1980.[7] The first aim of this method is the eradication of microscopic residual disease. It has the benefit of higher concentrations of drugs delivered locally to the tumour site while preventing the systemic toxic effects compared with intravenous administration. The efficacy of a drug is calculated by the ratio of the peritoneal cavity area under the concentration/time curve (AUCc) to the plasma area under the concentration/time curve (AUCp).[8] This ratio is between 250-1400 for 5-Flourourasil, 12-20 for cisplatin and 75-80 for mitomycin-C.[2],[9],[10] The efficacy is increased with the slow absorption rate of the cytotoxic drug. Hydrophilic drugs like 5-Flourourasil, cisplatin and mitomycin-C are absorbed very slowly from the peritoneal surface so they are the most useful drugs for IHCP. Beyond this the direct tumour absorption of drugs occurs to a level of 5 mm beneath the tumour surface, that means tumour nodules exceeding 5 mm are not suitable for IHCP.[7],[9],[11],[12] In this technique hyperthermia also enhances the efficacy with its own cytotoxic effect by maximizing the diffusion of the drugs to the tumoral nodules. In gastric cancer IHCP can also be used as neoadjuvant aim for down-staging but the most preferential use is the adjuvant route. Takahashi and Hagiwara used activated carbon particles in the peritoneal cavity, which adsorbed a large amount of mitomycin-C in gastric cancer patients with definite serosal involvement.[13],[14] They found 14 and 18% of survival advantage in 2 and 3-year times respectively compared with control groups. In other studies that used cisplatin or mitomycin-C in early postoperative intraperitoneal chemotherapy, statistically significant survival advantages were found against control groups and it was determined that this advantage appeared especially in Stage III diseases.[3],[15],[16],[17] Fujimura et al reported 40% complete remission and 67% and 40% of 1 and 2-year survival rates after IHCP in gastric cancer patients with peritoneal seeding.[18],[19] Fujimoto et al also reported the results of 141 patients with locally advanced gastric cancer who underwent cytoreductive surgery, and 71 of them also underwent IHCP.[20] In this trial it was seen that in the IHCP group the 2, 4, and 8 year-survival rates were 88, 76, and 62% while in control group they were 77, 58, and 49% respectively. Hamazoe et al also found 64% 5-year survival rates of patients in IHCP.[21] Similarly, long-term survival rates of 25-50% have also been described in patients who underwent cytoreductive surgery and IHCP, and in these studies it seems that the survival advantage of IHCP is better than intraperitoneal chemotherapy alone.[22],[23],[24] The most important reasons behind this result are the use of hyperthermia and maximum drug concentration in IHCP. With the help of these data the treatment algorithm has been evolved for the management of operable gastric cancer was determined in 1996 by Kelsen.[25] Today this algorithm is still valid, but has been modified to included IHCP [Figure - 2]. In the use of IHCP there are also some restrictions in that IHCP only treats peritoneal disease so it is contraindicated when extraperitoneal metastases are found. Beyond this, macroscopic cytoreductive surgery must be performed before IHCP. The residual disease or the nodules in the peritoneal cavity must be smaller than 5 mm, and there must be no adhesion in the peritoneal cavity that restrict the homogeneity of distribution of the cytotoxic agents. In this study, although the number of patients is small, the effective control of local peritoneal recurrence (10%) and improved overall and disease free survival have been encouraging. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04071f2.jpg] [is04071f1a.jpg] [is04071f1b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}