 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 5, September-October, 2004, pp. 281-285 Original Article A randomized comparative study of micronised flavonoids and rubber band ligation in the treatment of acute internal haemorrhoids Sandhu PushpinderS, Singh Karam Department of General Surgery, Govt. Medical College & Rajindra Hospital, Patiala Code Number: is04072 ABSTRACT BACKGROUND: Haemorrhoids is a common disease affecting people of all ages and both sexes. Though there is a consensus on the treatment of 3rd and 4th degree haemorrhoids, there is still confusion regarding the ideal treatment for Ist and IInd degree haemorrhoids.AIMS: To compare the safety, efficacy, advantages and disadvantages of Rubber Band Ligation and Micronized Flavonoids in the treatment of acute internal haemorrhoids and the compliance and acceptability in patients. SETTINGS AND DESIGN: One hundred patients of acute internal haemorrhoids, with chief complaint of bleeding per rectum due to internal haemorrhoids, presenting in the outdoor patient department of a tertiary care hospital were randomly subjected to Rubber Band Ligation or Daflon 500 mg (50 each). METHODS AND MATERIALS: One hundred patients of acute internal haemorrhoids were treated with Rubber Band Ligation or Daflon 500 mg (50 each). The outcome measures were relief from bleeding and the total days taken for it. STATISTICAL ANALYSIS USED: Categorical data was compared by the standard error of difference in proportions and the changes were compared by the t test. Significance was defined by P<0.05. RESULTS: 84% of patients on Daflon 500 and 60% of patients undergoing Rubber Band Ligation were completely cured (P<0.01) on the 7th day but this statistical significance was lost during consequent follow-up. CONCLUSIONS: Daflon gives rapid relief from symptoms of acute internal haemorrhoids as compared to Rubber Band Ligation but the long duration of treatment and its high cost leads to poor patient acceptability and compliance. KEY WORDS: Rubber Band Ligation, Daflon, internal haemorrhoids INTRODUCTION Haemorrhoids is an affliction as old as mankind itself. Since man assumed an erect posture, he has been punished with a protruding painless bleeding mass at the anus. They have been defined as a mass of dilated tortuous veins in the anorectum involving the venous plexus of the area.[1] Depending on the symptoms produced the haemorrhoids are classified in degrees as following:[2] 1st.
Bleeding, with haemorrhoids that prolapse into but not out of the anal
canal. Milligan et al described haemorrhoidectomy in 1937[3] and it is generally agreed that all patents with IVth degree haemorrhoids and most patients with IIIrd degree haemorrhoids would be best advised to undergo this procedure.[4] The treatment of Ist and IInd degree haemorrhoids is more controversial. Sclerosant injection therapy, Lord′s procedure, Rubber Band Ligation, Infrared coagulation, Bipolar electro coagulation, Cryosurgery etc are some of the treatment modalities used for Ist and IInd degree haemorrhoids. According to Bayer[5] Rubber Band Ligation is a safe, cheap and convenient method and can save hundreds of hospitalization days. But Rubber Band Ligation is not flawless. The various disadvantages include:
In 1971, Daflon, which is 90% Diosmin and 10% Hesperidin (Daflon 500; Serdia Pharmaceuticals, India and Vinosmin; Elder Pharmaceuticals, India), was introduced in France by Bensaude et al[8] for the treatment of haemorrhoids and other capillovenous diseases. Daflon acts at the following levels:-
Side-effects of the drugs are limited and according to Meyer,[11] mild gastrointestinal and autonomic disturbances are seen in 10% cases. The micronized flavonoid, Daflon, has been compared with placebo,[12],[13] with non-micronized Diosmin[14] and with fibre and Rubber Band Ligation.[15] This study was therefore done to compare the most commonly used treatment for Ist and IInd degree haemorrhoids i.e. Rubber Band Ligation with Daflon 500. MATERIALS AND METHODS The ethics committee of the medical college had approved the study. The study was prospective and was conducted on 100 patients presenting in the outpatient department of a tertiary level hospital. The patients selected were of both sexes and above 18 years of age and had presented with the chief complaint of bleeding per rectum because of Ist and IInd degree haemorrhoids and with associated pain, tenesmus, discomfort, pruritis or anal discharge. The status of the internal haemorrhoids was confirmed by proctoscopy. The criteria for non-inclusion in the study were other anorectal diseases, inflammatory bowel disease, pregnancy or any previous history of surgery for haemorrhoids. Written informed consent was taken from all patients and after the preliminary assessment of patients i.e. detailed history of the disease and general and systemic examination, the patients were subjected to a few baseline investigations (haemoglobin, bleeding time, clotting time, urine complete examination). The patients were randomly subjected to Daflon or Rubber Band Ligation depending on their choice, after discussing the advantages and disadvantages of both methods with them. Fifty patients each were either given Daflon 500 mg or underwent Rubber Band Ligation. Daflon 500 mg was given in the dose of 3 tablets twice daily, after meals, for three days followed by 2 tablets twice daily from the 4th day to the 7th day. On the 7th day the symptoms and any relief was recorded and the dose was further decreased to one tablet twice daily for the next 83 days (total duration of treatment 90 days). Consequent follow-ups were done on the 15th, 30th and 90th day. In patients undergoing rubber band ligation, no prior preparation was required and the procedure was done in the outpatient department. Only one pile was banded at a time and in patients with multiple piles, every other pile was banded after a week′s interval. Follow-up was done on the 15th, 30th and 90th day. No other preparation like stool softener was given. The patients were labelled cured (C), improved (I), unchanged (U) or worsened (W) depending on the relief from their symptoms. Cured
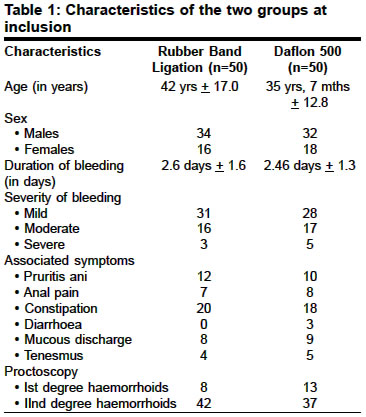
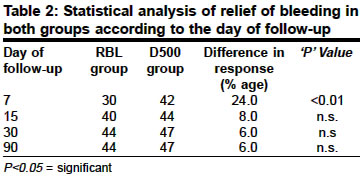
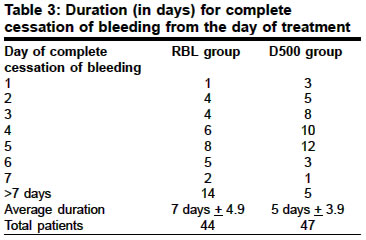
(C) - Absolute disappearance of symptoms. Statistical Analysis The primary outcome measure was the number of patients with no bleeding on the 7th day, while the secondary outcome measure was the average days taken for complete cessation of bleeding in both groups. Categorical data was compared by the standard error of difference in proportions and the changes were compared by the t test. Significance was defined by P<0.05. Apart from primary outcome measure and secondary outcome measure, statistical comparison between relief obtained from associated complaints was also made and conclusions drawn. RESULTS The majority of the patients (31%) were in the age group of 21-30. Sixty-six per cent were males and 34% were females [Table - 1]. The average age of the patients in the Rubber Band Ligation group was 42 yrs +17.0 and in Daflon 500 group was 35 yrs, 7 months +12.8 (the difference of age in the two groups has no statistical significance as the patients were randomly subjected to either Daflon or Rubber Band Ligation, depending on their choice). Fifty-nine per cent of the patients had mild bleeding in the form of drops of bright red blood during the act of defecation, while 33% patients had moderate bleeding i.e. in the form of streak of bleeding during defecation and 8% of patients had severe bleeding i.e. in the form of stream or pool of blood during defecation. A record of associated symptoms i.e. pruritis ani, anal pain, constipation, diarrhoea, mucous discharge per rectum, and tenemus was kept. On proctoscopy, Ist degree haemorrhoids were found in 21% of patients (8 patients in the Rubber Band Ligation group and 13 in the Daflon 500 group), and 79% of patients had IInd degree haemorrhoids. In the Daflon 500 group 84% of patients (n=50) gave history of complete cessation of bleeding on the 7th day of treatment while only 60% of the patients in the Rubber Band Ligation group were cured of the symptoms, 7 days after the last haemorrhoid had been ligated [Table - 2]. This difference was statistically significant (P<0.01) but this significance was not maintained in the later days of the follow-up. A record of relief obtained from other symptoms was also kept. The relief obtained was statistically significant on the 7th and 15th day of follow-up (e.g. in case of pruritis ani P=<0.02 on the 7th day of follow-up, in favour of Daflon 500) but this significance was lost in the subsequent days of follow-up. The secondary outcome measure was the average days taken for the complete cessation of bleeding in both the groups. The average days for the cessation of bleeding in the Rubber Band Ligation group was 7 days + 4.9 and in the Daflon 500 group was 5 days + 3.9 [Table - 3]. This difference was statistically significant (P<0.001). In the Rubber Band Ligation group, two patients relapsed by the end of the study while in the Daflon 500 group one patient had relapse of symptoms and all these 3 patients had to undergo haemorrhoidectomy. DISCUSSION The alimentary tract terminates at the anus, which is preceded by the rectum. The complex of these two is known as the anorectum. The wall of the anorectum contains the terminal branches of the superior haemorrhoidal artery in the internal haemorrhoidal plexus and the enlargement of these results in internal haemorrhoids. The three principal haemorrhoids are found at the 3,7 and 11 o′clock position.[16] There is a consensus on the treatment for 3rd and 4th degree haemorrhoids and it is haemorrhoidectomy. The best treatment for Ist and IInd degree haemorrhoids though is still an enigma. The various modalities of treatment include sclerosant injection therapy, Lord′s procedure of anal dilatation, cryotherapy, infrared coagulation, laser therapy, direct electrocautery, bipolar coagulation and Rubber Band Ligation. According to Bayer,[5] Rubber Band Ligation is the safest, cheapest and the most convenient treatment. Daflon 500 focuses on the inflammatory pathology of haemorrhoids by increasing the duration of the contraction of veins and local lymphatic drainage[17] and by decreasing the synthesis of prostaglandins like PGE2 and thromboxane B2. The anti-inflammatory effects of Daflon are reflected in the reduction of capillary hyperpermeability[18] and fragility in controlled clinical studies. In our study acute internal haemorrhoids were most common in the 3rd decade of life (75%). The male to female ratio was 1.9:1. The average duration of bleeding at presentation was 2.6 days + in the Rubber Band Ligation group and 2.46+1.3 in the Daflon group. This suggests that for most patients of acute internal haemorrhoids, haemorrhoidal bleeding and other associated symptoms constitute an emergency and they would prefer a rapid relief from it. Daflon 500 mg by the virtue of its anti-inflammatory properties, led to rapid relief from the primary complaint i.e. bleeding per rectum. The difference in patients who were totally relieved of bleeding per rectum, which was the primary outcome measure, on the 7th day of treatment was statistically significant among the two groups i.e. P<0.01 [Table - 2]. This significance though was lost during the subsequent follow-up. The same pattern of relief was also seen in the associated symptoms. Bleeding was the presenting complaint in all 100 patients. The average number of days for the cessation of bleeding in the Rubber Band Ligation group was 7 days + 4.9 and in the Daflon 500 group was 5 days + 3.9 [Table - 3]. This difference was statistically significant (P<0.001). This indicates that a patient with a presenting complaint of haemorrhoidal bleeding and one seeking rapid relief from it would be more satisfied with Daflon 500 mg than Rubber Band Ligation. By the end of the study 94.0% patients in the Daflon 500 mg group were satisfied with the treatment while this figure was 89% in case of the Rubber Band Ligation group. This difference was statistically insignificant. CONCLUSIONS We conclude that Daflon leads to the rapid cessation of haemorrhoidal bleeding, alleviation of the associated symptoms and gives objective relief from acute internal haemorrhoids. In the present study, Daflon was very effective in the first 30 days of treatment and led to the rapid relief of various associated symptoms. Daflon was more effective than Rubber Band Ligation during the acute phase of the disease. A limitation of the drug is the lack of patient compliance due to the long duration of treatment and the high cost of the drug. The safety of the drug has already been proved but more studies need to be done to see if the total dose of Daflon can be increased so as to increase the response rate and decrease the duration of treatment. A decrease in the cost of the drug would also be welcome. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04072t1.jpg] [is04072t3.jpg] [is04072t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}