 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
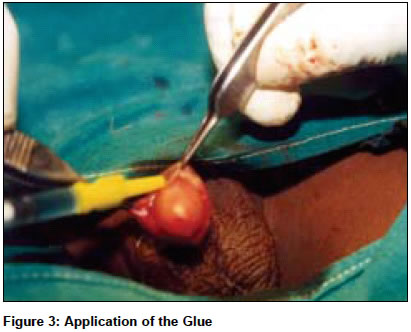
Indian Journal of Surgery, Vol. 66, No. 5, September-October, 2004, pp. 286-288 Original Article Sutureless circumcision: Wound closure after circumcision with cynoacrylate glue - A preliminary Indian study Sharma PradeepP Department of Surgery, Hon. Associate Professor in Surgery, Bharati Vidyapeeth Medical College & Hospital, Pune Code Number: is04073 ABSTRACT Alternative methods of wound closure after formal circumcision have been studied to decrease the repair time and complications, and to improve cosmesis. This was a prospective non-comparative preliminary clinical study involving 15 patients where Cyanoacrylate glue was used as a tissue adhesive for wound closure after formal circumcision. It was found that the repair time was short, complication rate was low and the cosmesis was good. Thus Cyanoacrylate glue may be considered as a useful alternative to suture closure for circumcision wounds.KEY WORDS: Sutureless, circumcision, Cyanoacrylate, glue INTRODUCTION Circumcision is a commonly performed surgery all over the world by general surgeons, urologists, paediatric surgeons, physicians, family physicians, midwives and even quacks. It is one of the oldest operations documented nearly 2500 BC and has many controversies associated with it.[1],[2] Nearly 1.2 million newborn males are circumcised yearly in the United States and nearly 30,000 in the UK.[1],[3] Currently one-sixth of the world′s male population is circumcised, mostly on religious grounds. In India the incidence of circumcision in the general population is 33%.[4] The complication rate after circumcision is 0.2% to 6%.[5],[6] There is probably no other surgical procedure that is performed by so many specialists, yet the overall results are excellent.[7] Haemorrhage and infection are the most common complications, followed by wound separation, recurrent phimosis, preputial adhesions, and unsatisfactory cosmesis due to scar formation. Recently, alternative wound closure methods have been studied to decrease the complication rate and repair time, and to improve the cosmetic outcome. Tissue adhesives like Cyanoacrylate have recently invoked a lot of interest in the field of wound healing. By undertaking this clinical study we thought of using Cyanoacrylate glue to close circumcision wounds. MATERIALS AND METHODS Fifteen healthy young males from the age of 2 yrs to 25 yrs, during a period Jan 2003 to Dec 2003 in one of our surgical unit comprised the study group. There were no exclusion criteria. The indications for surgery were congenital or acquired phimosis, recurrent balanoposthitis and religious reasons. Appropriate blood tests were performed and consent for the surgery was taken. The operation was performed under local anaesthesia (Dorsal Penile Nerve block) in the older group while general anaesthesia or local anaesthesia was supplemented with sedation (Ketamine Hydrochloride) in the younger group. The technique of dorsal slit followed by free-hand cutting all around with sharp scissors was used in all the cases [Figure - 1]. The outer layer of the foreskin was retracted back and meticulous haemostasis was done with the help of bipolar cautery [Figure - 2]. The cut edges were approximated with McIndoe forceps and the glue was applied [Figure - 3]. In some cases stay sutures with 4-0 chromic catgut placed 90 degree apart helped the application of the glue. The glue was applied meticulously and allowed to harden or polymerize [Figure - 4]. Leakage of the glue between the edges was avoided as it would delay the healing. A small gauze dressing was then applied so that the hardened glue does not catch the undergarments. All the patients received a 5-day course of 1st generation Cephalosporin Cephadroxil (considering its proximity to the urinary orifice) and analgesic Ibuprofen and Acetaminophen in appropriate doses. All the patients were discharged on the same day and followed at the outpatient department on the 5th, 10th, 15th, 30th and 90th day. Bathing over the operative site was permitted from the 5th day onwards. RESULTS The age of the patients ranged from 2 to 25 years. Indications: The average time taken for the procedure was 12 min (8 min to 15 min). The average healing period and falling away of the hardened glue was between 13 days to 28 days with a mean of 21 days. (The frenular junction is the last area to heal and usually takes a longer time). Complications: No major complication was seen. Minor wound separation was observed in 2 cases; however the raw area healed without any surgical intervention. DISCUSSION There are many techniques of circumcision but they can be broadly classified into four types: dorsal slit and free-hand cutting, using shield, clamp and sleeve excision. All the techniques have their protagonists. Cynoacrylate adhesives are monomers that polymerize and form strong bonds via an exothermic reaction in the presence of body fluid or tissue. These adhesives have been used to treat skin lacerations with favourable results. The Cyanoacrylates are bactericidal, chemically stable, easily stored making them useful clinically.[8] Recent clinical studies show a low rate of wound dehiscence, fewer wound infections and improved cosmetic outcome for wounds approximated with tissue adhesives. The Cyanoacrylates were developed as an alternative to sutures and have gained increased clinical popularity due to ease of application, decreased scarring, decreased pain, and as they are more efficient and provide finer cosmesis compared to sutures. Also, there is no discomfort as seen with the sutures getting adhered to or snagging the clothing and dressings.[3] Experimental studies in a rat model using Cyanoacrylate glue showed wound breaking stress comparable to that of suture closure. In addition, histological evaluation of tissues healed in the presence of the Cyanoacrylate showed normal wound-healing characteristics.[2] The Cyanoacrylates have been advocated for small, low-tension surgical incisions in the paediatric population. Circumcision wounds are small and low-tension and hence ideal for the use of these adhesives. Cheng and Saing reported no statistically significant difference in the rate of wound inflammation, infection, bleeding, dehiscence or cosmetic appearance of circumcision incisions repaired with N-butyl-2-cynoacrylate compared with suture approximation.[9] Zafar et al reported that the N-butyl-2-cyanoacrylate closure of circumcision wounds is technically easier with improved cosmesis and adequate tissue approximation.[3] There is decreased scarring and no lumpy contour. The stitch marks associated with sutures are also absent. This method also obviates the use of traditional dressings like Tincture Benzoin, Paraffin tulle or Sofra Tulle many of which are incorporated within the sutures to keep them in place and hence associated with pain during their removal.[10] There were no major complications in our study though the number was small. Even the wound separations which occurred were in the early part of the study and were due to faulty application of the glue. The cosmesis was better as there were no suture marks or lumpiness. Being sutureless may also increase the acceptance of the procedure. There are some demerits of this procedure like the availability of the glue in remote areas, storage problems due to short shelf-life outside refrigeration (the glue hardens at temperature above 25°C). Cost-wise, it is marginally higher to the suture closure (Cost of 0.25 ml of glue is Rs. 125 compared to a 4-0 catgut which is Rs. 110). However, a randomised controlled trial needs to be done to validate the benefits. CONCLUSIONS I conclude that circumcision wound closure is feasible with the glue, is easier and is associated with less pain. It requires less nursing care in the postoperative period. The complication rates are low and the cosmesis is excellent. Care should be taken to approximate the edges well before the application of the glue. Thus it can be considered as an alternative to suture in the circumcision incision closure. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04073f3.jpg] [is04073f2.jpg] [is04073f4.jpg] [is04073f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}