 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
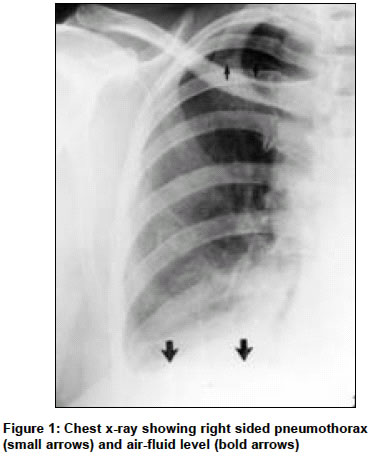
Indian Journal of Surgery, Vol. 66, No. 5, September-October, 2004, pp. 294-296 Case Report Spontaneous pneumothorax - A rare complication of laparoscopic cholecystectomy Kaushik Robin, Attri AshokK Department of General Surgery, Government Medical College and Hospital, Chandigarh Code Number: is04077 ABSTRACT We report the case of a 50-year-old lady who developed spontaneous right-sided pneumothorax during laparoscopic cholecystectomy. This was detected intra-operatively by a fall in her oxygen saturation and was confirmed by clinical examination. Postoperative chest X-ray also documented right-sided pneumothorax. The pathogenesis and management of this rare but potentially life-threatening complication is briefly discussed.KEY WORDS: Laparoscopy, pneumoperitoneum INTRODUCTION Although first described in 1939, spontaneous pneumothorax remains an extremely uncommon complication of pneumoperitoneum, with a reported incidence of 0.01-0.4%.[1],[2] It is important to be aware of this rare but life-threatening complication not only for diagnosis purposes, but also for management, since treatment can vary from simple close observation in a stable patient to immediate chest tube thoracostomy in an unstable one. Such a case who developed spontaneous right-sided pneumothorax during laparoscopic cholecystectomy is presented and its pathogenesis and management reviewed. CASE REPORT A 50-year-old female patient with symptomatic cholelithiasis (for a period of 2 years) was admitted for elective laparoscopic cholecystectomy (LC). Her routine haematological and biochemical investigations (including liver functions) were within normal limits. Ultrasound examination of the abdomen had revealed multiple calculi within the gall bladder, with normal common duct and pancreas. After induction of anaesthesia, LC was performed by a standard four-port approach using monopolar cautery. The infra-umbilical trocar was placed by an open method and pneumoperitoneum was created. The other three ports were placed under vision. LC proceeded without any technical difficulty. After about 45 minutes of starting LC, when the gall bladder was being dissected off the liver bed, the anaesthetist noticed a fall in the oxygen saturation progressively from 100% to 88%. The patient was shifted onto manual ventilation, and the possibility of pneumothorax was entertained as there was difficulty in ventilating the patient manually. Auscultation revealed a reduction in the breath sounds on the right side. As the patient was otherwise stable (normal pulse rate, blood pressure, end-tidal CO2 and ECG tracing), LC was completed and the gall bladder delivered through the epigastric port. Although the surgery had been uneventful, we performed laparoscopy again to visualize the diaphragm, but no rent or injury could be identified. After lavage, the pneumoperitoneum was deflated and the surgery completed. The saturation had risen to 95% by the end of the surgery, although it did not reach its pre-surgical value of 100%. There was an appreciable improvement in the breath sounds on the right side as compared to the earlier status. The patient was extubated and shifted to the recovery room. A chest X-ray was performed within one hour of extubation [Figure - 1]. This revealed pneumothorax towards the apex, with an air-fluid level on the right side. As the patient was maintaining near normal saturation and stable vitals, no therapeutic intervention was thought to be necessary. She remained under close observation during her hospitalization, and was discharged on the 3rd postoperative day when her chest X-ray revealed a fully expanded lung and clear costo-phrenic angle on the right. DISCUSSION Pneumothorax can develop during LC either by direct injury to the diaphragm or spontaneously. Direct injury to the diaphragm usually occurs when the gall bladder is being dissected off the liver bed, since upward traction of the gall bladder and the right lobe of the liver brings the undersurface of the diaphragm in close proximity to the working area. Such an injury may produce life-threatening tension pneumothorax by virtue of the rent in the diaphragm acting as a flap that opens during inspiration and closes during the inspiratory phase of ventilation.[2] However, the exact mechanism of the occurrence of spontaneous pneumothorax remains by and large unknown till date. It has been postulated that air may enter the mediastinum through the aortic and oesophageal hiatuses of the diaphragm, later rupturing into the pleural space. Congenital weak points or defects of the diaphragm (pleuroperitoneal hiatus, outer crus, oesophageal hiatus), lack of adequate muscle fibres of the sternal, costal or lumbar parts of the diaphragm, their weakness, or failure of their fusion can also lead to weak points that may rupture secondarily to the continuous high pressure of pneumoperitoneum.[1] One should suspect pneumothorax during surgery even in the absence of physical signs when there occurs an increase in the airway pressures, a decrease in pulmonary compliance, when there is an unexplained fall in the oxygen saturation, or when there is unexplained hypoxia, hypercarbia, or haemodynamic instability. If recognised during the beginning or middle of surgery, the treatment consists of deflating the abdomen, performing a tube thoracostomy, and then proceeding with the surgery if the patient remains stable. If detected towards the end of the procedure in a stable patient, the operation should be completed and nothing further needs to be done since the carbon dioxide in the pleural cavity gets rapidly reabsorbed after deflating the abdomen.[1] To conclude, pneumothorax is a rare complication of pneumoperitoneum. With the increasing use of laparoscopy as a diagnostic and therapeutic tool, it is important to be aware of this potentially life-threatening complication and its management. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04077f1.jpg] |
| |||||||||

{kind=link}