 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
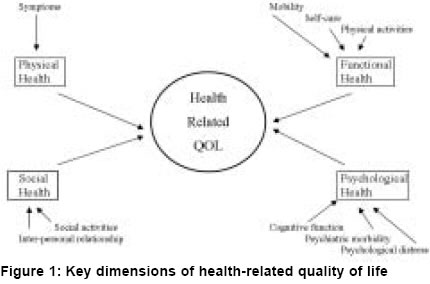
Indian Journal of Surgery, Vol. 66, No. 6, November-December, 2004, pp. 323-335 Review Article Health-related quality of life and its assessment in GI Surgery Sharma Dhananjaya Govt. NSCB Medical College and Allied Hospitals, Jabalpur - 482 003 Code Number: is04085 KEY WORDS: Quality of life, health-related quality of life, GI surgical procedures. When you can measure what you are speaking of and express in terms of numbers, you know something about it; when you can not express it in numbers, your knowledge is of a meager kind" - Lord Kelvin (Famous Physicist) Interest is increasing in the measurement of quality of life (QOL) in clinical research but most often lack of information about the clinical significance and advantages of these studies are impediments to their full and proper use. These issues and problems are discussed in this review. The first half of this article reviews the frequently asked questions about quality of life studies and the second half discusses clinically relevant issues, vis-a-vis, QOL and its assessment in GI Surgery. WHAT IS HEALTH-RELATED QUALITY OF LIFE? Modern medical science has ensured significant progress in the diagnosis and treatment of disease. Traditionally, the success of treatment has been measured by biomedical/clinical end points like survival (overall or long-term, specific or corrected survival, disease-free survival, recurrence-free survival), response rates, time to progression, relapse or treatment failure, and surgery-related items like mortality, duration of hospital stay and complications etc. However, diseases and their treatment may have an impact not only on survival (quantity of life), but also on the well-being of the individual, the ′quality of life′. Effort is now being made to gauge these consequences. QOL is a multidimensional dynamic concept that has developed from the need to estimate the impact of diseases, which includes economic welfare, characteristics of community and environment, and health status. In the purest sense, quality implies subjective evaluation by the individual. QOL is variously referred to as patient-assisted outcome measure, health status, and functional status or just as outcome measure. Aspects of health status that a person values overlap with the components of QOL and are called Heath-Related Quality of life (HRQOL). QOL and HRQOL are often used interchangeably, often with little distinction between the two concepts, giving rise to confusion in this area of research. There is a need to distinguish between global well-being and health-related well being although health is one of the strongest determinants of global QOL. Key dimensions of HRQOL are physical functions, sensations, self-care/dexterity, cognition, pain/discomfort and emotional/psychological well-being i.e. "all within the skin" [Figure - 1]. Therefore, HRQOL is more appropriate for our use as health workers can influence by improving patient′s illness. There is increasing consensus that "QOL is important". However, what exactly is QOL? Defining and measuring this elusive concept is a major challenge to clinicians, leading to different definitions as well as different scales for its measurement. The term QOL has become a bandwagon concept for all those human needs, which are often neglected in a society dominated by technology. As a rule, the term QOL is used in medical research for characterizing an individual′s QOL from his own subjective perspective, as contrasted with the professionals′ objective evaluation of the health status of the individual.[1] WHO has defined QOL as "an individual′s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns. It is a broad ranging concept affected in a complex way by the person′s physical health, psychological state, level of independence, social relationships and their relationships to salient features of the environment".[2] An excellent review of various global and specific definitions of health and QOL has been recently published.[3] Another concept to emerge from these deliberations is the Quality Adjusted Life Years (QALYs), which stemmed from the presumption that a treatment plan improving QOL without survival benefit will be preferred by the patient over a treatment plan with survival benefits but serious discomfort. An increasingly used extension of QALY is Quality adjusted Time Without Symptoms or Toxicity (Q-TWIST): which obviously means quality symptoms-free time without adverse effects of treatment. HRQOL is a relatively new addition to the tools that clinicians use to gain a better understanding of the impact of disease and its treatment. The science of QOL assessment is a vibrant, although young discipline. The history of the term "Quality of life" is quite short: it was first used in 1960 and became a key word for medical literature retrieval at ′Medline′ in 1977. The young science got a boost with the development of the speciality journal "Quality of Life Research" in 1993. WHY MEASURE/ USE HRQOL? There are many valid reasons for measuring HRQOL:
The final reason for measuring HRQOL is that such measures have repeatedly shown to work for improvement in patients′ management. The biggest advantage of QOL studies is that now patient′s perspectives and views are increasingly being heard and paid heed to by the clinicians; who in turn have become more sensitive to patients′ needs and have learnt to communicate better. This can be truly called ′moving beyond survival′, a much needed step forward in the treatment philosophy. Science has increasingly ensured longevity of life, the next goal of researchers is to identify ways to enhance QOL. Survival alone, is now regarded as insufficient, only a treatment which improves QOL is regarded as effective even if it is without survival benefit. Interest in QOL assessment in clinical research has been growing fairly rapidly as it is propelled by a growing concern for the quality of healthcare. QOL is now increasingly being recognized as an end point, perhaps at par in importance with survival. There is often a compromise between disability and survival, and it is this compromise which justifies the assessment of HRQOL in the evaluation of healthcare, and perceived QOL reflects the size of gap that the individuals see between their actual situation and that to which they aspire. HOW IS HRQOL MEASURED? HRQOL data is collected using structured multi-item questionnaires consisting of a number of questions which tap various dimensions of HRQOL (to estimate daily function) and allow the clinician to assess the impact of disease and its subsequent treatment upon the patient′s daily life. The answers to these items are then given a score, thereby converting qualitative information into quantitative data. When one global score represents QOL it is called a quality of life index. The questionnaire may be administered by an interviewer, face-to-face or constructed in simple and straightforward language and may be completed by the patient himself. HOW TO DEVELOP A NEW HRQOL SCALE? Development of a new HRQOL scale is a multistage procedure:
WHAT ARE THE QUALITIES OF A GOOD HRQOL INSTRUMENT? Qualities of an ideal QOL instrument are acceptability (by patients, vis-à-vis their interest and relevance), feasibility (burden on the research worker), reliability and reproducibility (degree of measurement error and repeatability of performance even in the hands of different workers at different points of time), responsiveness (sensitivity to capture change over time), validity (ability to measure the variable it is supposed to measure, and detect even small clinically significant differences), interpretability (extent of meaning of the data generated) and usefulness (how it affects clinical management and policy). WHAT ARE THE DIFFERENT TYPES OF HRQOL INSTRUMENTS? There are two main types of QOL instruments: generic and specific. Generic instruments are designed to assess the many dimensions of health-related issues and are used for health policy research as they assess the impact of disease on mental/social functioning; specific instruments (domain/disease-specific, population-specific, function-specific, symptom-specific or ad-hoc scale pertinent to one study only) measure only a specific area of quality of life, rather than assessing quality of life globally. For instance, some of the commonly used cancer-specific scales are CARES (CAncer Rehabilitation Evaluation System), FACT-G (Functional Assessment of Cancer Therapy-General), FLIC (Functional Living Index: Cancer) and EORTC-QLQ-C30 (European Organization for Research and Treatment of Cancer-Quality of Life Questionnaire-Core 30). WHICH QOL INSTRUMENT SHOULD BE USED? Hundreds of different scales are available for the measurement of QOL, varying from seductively simple to very complex scales.[6] The choice of scale depends on the type of study being conducted. The optimum properties of a QOL scale are determined by the purpose for which it is put, in the same way that the selection of a surgical instrument is determined by its use. There is no such thing as a ′best scale′ in an absolute sense, only scales best suited to a particular purpose. Scales best suited for longitudinal purposes (clinical trials and audit) have different properties to those suited for cross-sectional studies (population and correctional studies and clinical use).[7] In a cross-sectional study, where quality of life is assessed at one point in time, useful information is obtained from a generic questionnaire. In a longitudinal study, where quality of life is assessed before and after an intervention, a disease-specific questionnaire should be used to measure responsiveness to change. It is noteworthy that the total score of a QOL questionnaire reflects the items that make up the questionnaire. Although different questionnaires seem to have strikingly similar items the balance between types of items can actually measure markedly different aspects of QOL.[8],[9] When selecting an instrument from those available it may happen that no one scale is ideal. If no scale is suited for a particular purpose, then researchers should consider developing a new one. Under these circumstances, the researcher needs to make a clinical judgement about suitability from those available, compromising between the three primary purposes: discrimination, evaluation and prediction. An excellent guide to the selection of a QOL instrument is now available.[7] Example of a simple scale: ′EuroQol 5-D′ survey measures QOL by a three tier simple questionnaire measuring 5 domains: mobility, self-care, usual activities, pain/ discomfort and anxiety/ depression, in this particular order.[10] These 5 domains are measured on a scale of 1-3, with 1 signifying no problem and 3 signifying maximum degree of problem. For example, "11223" means: 1 = No problem in walking about By and large, because of the requirements, QOL questionnaires have to be comprehensive, detailed and multidimensional. A premium cannot be placed on brevity at the expanse of clinical utility. Logic dictates that a complex problem will require a complex solution. Commonly used scales, e.g. EORTC (European Organization for Research and Treatment of Cancer) and GIQLI (Gastro-Intestinal Quality of Life Index) questionnaires have been successfully translated and used in many languages. WHO SHOULD MEASURE HRQOL? Correlation of clinicians′ and patients′ perception of QOL has been notoriously poor. Proxy respondents appear to underestimate the full effect of chronic illness on QOL, although patients′ partners seem to have a better (than clinicians) idea about the patients′ QOL.[11] Cogent to this discussion is that most investigations claiming to measure QOL, in fact measure physical functioning which has to be differentiated from QOL, which is a completely subjective evaluation and related to a patient′s personality. This point has been underlined by the example given by Cohen et al about a patient with advanced cancer who emphasized that her QOL has improved over the preceding week, explaining: "Nothing that is happening to me has improved, in fact, physically I am feeling worse. What is different is how I am taking it."[12] McKay wrote a poem in 1925: "If we must die; let us nobly die". The message is about dignity of living as well as about dying with dignity; these being very subjective and personalized evaluations by individual patients. Therefore, even if two patients have the same physical condition, their QOL scores can dramatically vary, giving rise to studies classifying patients according to their "egograms". This is the reason why ethically as well as scientifically, the patient is the only person who should be judging his/her QOL. Any proxy judgement by a clinician/nurse or healthcare economist will not give the right picture. The primacy of a patient′s perspective can never be undermined, as QOL is a reflection of what is important to the patient. "How is the patient?" QOL studies open the door to the patient′s perspective in answer to this question. The clinical relevance of this point is that any improvement in clinical or laboratory indices, unless translated into improved QOL for the patient, is fallacious. THE ISSUE OF QOL IN GI SURGERY AND THE SURGEONS′ ROLE IN QOL STUDIES:[13],[14],[15] The principal criteria guiding the patients′ acceptance of treatment are most often the patients′ subjective feelings i.e. the quality of their lives. As the surgery asks patients to trade present discomfort and risk for future gains, in gauging the achievements of surgical treatment it is important to try to measure the quality of functional result vouchsafed to the patient. Another reason is that "surgery is forever" and cannot be undone. Broadening the choice of endpoints beyond traditional, so-called "hard" variables, and including QOL in surgical studies has advantages for both surgeons and patients. Because the impairments of function that may occur after different operations vary considerably, an operation-specific assessment of QOL for each type of surgical procedure is essential. Until now most of the QOL studies have been performed by non-surgeons with psychometric support, but it is time for the surgeons to provide leadership in QOL studies. Performing these studies will allow the surgeons to bridge another divide, open doors to showing more sensitivity, leading to better communication with their patients. A free and frank discussion, about QOL gains, as a benefit of surgery, at the time of counselling will go a long way in ensuring that the patients′ perspectives get their rightful place in decision-making. So the answer to the question, QOL measurements: who benefits? is that everyone benefits, surgeons as well as patients. OESOPHAGEAL SURGERY Surgery for Gastro-oesophageal reflux disease Various QOL scales have been used for Gastro-oesophageal reflux disease (GERD); these are Quality of life in reflux and dyspepsia (QOLRAD), Gastro-oesophageal reflux disease Health related QOL (GERD-HRQOL) and the ubiquitous GIQLI. It has been consistently shown in many studies that the QOL of patients after laparoscopic or conventional surgery for GERD improves and is close to the level expected in a healthy individual.[16],[17],[18] Many reports have proved that heartburn score, dysphagia score, regurgitation scores and global QOL scores are superior after laparoscopic fundoplication compared with medical management.[19] Both partial and complete wrapping offer an effective form of therapy for reflux disease with over 85% patient satisfaction, however, partial fundoplications have been found to be associated with fewer mechanical side-effects.[20] A recent, randomised, controlled clinical trial has shown that posterior partial fundoplication functions better than an anterior one but without explaining the reason for this.[21] Surgery for GERD is often advised as a means to provide a long-term benefit and eliminate the need for medications, however, reflux symptoms may persist even after surgery due to functional dyspepsia and may spoil the expected outcome in a few patients.[22] Currently, 3 endoscopic techniques are available for the control of reflux: endoscopic suturing, endoscopic radiofrequency treatment of the LES, and injection of ethylene vinyl alcohol polymer into the LES. As yet, it is a bit too early to compare their outcomes with standard surgery, which remains the gold standard. Surgery for achalasia No currently available treatment for achalasia, whether medical or surgical, can restore normal oesophageal motility, but surgical management of achalasia offers excellent results in most patients with QOL scores matching the controls in the long follow-up of 18 months.[23],[24] Surgery for oesophageal carcinoma Dysphagia is a troublesome symptom which affects all aspects of quality of life.[25] Oesophagectomy remains a formidable surgical procedure and when performed for oesophageal carcinoma results in a negative impact on QOL; but this effect is transient for patients who survive for 2 or more years. After this period their general quality of life is similar to that of healthy individuals of the same age. This finding should be considered when selecting patients for surgery.[26],[27] Of the several factors analysed, only tumour recurrence (P<0.01) and anastomotic stricture (P<0.05) lower the quality of life significantly.[28] Factors affecting late functional outcome were analysed in two studies and it was shown that patients who had a cervical anastomosis had significantly fewer reflux symptoms (P<0.05). Dumping syndrome occurred more frequently in younger patients (P<0.05) and women (P<0.01).[29],[30] Duodenogastroesophageal reflux may eventually be the major cause of morbidity 10 years after oesophagectomy for carcinoma. Traditionally, it has been taught that posterior mediastinal reconstruction be used when curative resection is definitely achieved in order to avoid possible complications by local recurrence. However, in the palliative situation, the retrosternal route of reconstruction can be used as the functional disadvantages have no negative effect on the quality of life. Surprisingly, a meta-analysis has shown that posterior and anterior mediastinal routes of reconstruction are associated with similar QOL outcomes after oesophagectomy for cancer.[31] The logic of using stent placement as the first choice for inoperable malignant stenosis or oesophageal fistula is confirmed in many studies as following endoscopic palliation of dysphagia, quality of life can be maintained and improvement of swallowing is seen.[32],[33] It has been shown that patients treated by oesophagectomy reported significantly better physical, emotional, cognitive, and global health scores than those in the palliative treatment group.[34] Wong et al have shown that even a palliative oesophagectomy provides enhanced QOL with marked symptomatic benefits and enjoyment of daily living comparable to that observed following curative resection.[35] After curative surgery, most patients have a good appetite, take ordinary solid foods, and are satisfied with the daily amount of foods. However, about one-third of the patients complain of passage disturbance on swallowing, abdominal pain or diarrhoea after a meal. In these patients symptom management should focus on symptoms that interfere with the patients′ QOL. Further research should target the evaluation of specific interventions for symptoms. QOL after oesophagectomy, when analysed in detail, shows that the main psychosocial stress is less in the areas of anxiety and depression than in a loss of social activity and impairment of physical capacity. QOL assessment is an important tool to evaluate the adequate management of patients with oesophageal cancer. It has assumed even more importance in the light of evidence that supports a relationship between patient-rated scores of QOL and survival.[36],[37] GASTRO-DUODENAL SURGERY Acid Peptic disease Many research workers have studied QOL as outcome during the treatment of acid peptic disease. At one time, the major share of research was focussed on the effects of various types of vagotomies and their respective outcomes, but the advent of good anti-secretory agents have made routine surgery of acid peptic disease almost obsolete. Prior to the development of modern day QOL indices, outcomes of operations for peptic ulcer were measured in terms of Visick grading, which may be termed a forerunner of modern day QOL indices.[38] Now patients undergo surgery only for complications like peptic perforation. By using gastrointestinal quality of life index (GIQLI), it has been recently shown that peptic perforation does not result in any long-lasting impairment of QOL in survivors and the QOL improves to near normal in 6 months time after the perforation. It was seen that the overall GIQLI score as well as its GI core, GI disease-specific, psychological and physical and social components significantly increase over 3 and 6 months of follow-up, reflecting improvement in QOL as perceived by the patients.[39] Gastric oncosurgery Key issues in QOL after gastrectomy for carcinoma stomach are reservoir function of neo-stomach, absence of dumping and reflux and the ability to eat well to maintain/ gain weight. Control of these gastrointestinal symptoms is important to minimize impairment in QOL after gastrectomy. Measurement of QOL has been done by a variety of instruments and scales: Visick, Karnofsky, Spitzer′s QOL index, Cuschieri′s assessment, Gastro Intestinal Quality of Life Index and EORTC questionnaires. When restoring the continuity of the GI tract after gastrectomy, exclusion of the duodenal passage, although simpler, has altered the physiology of the duodenal bypass. Fortunately, dysmotility of the Roux limb is seen only in 10-30% cases and severe forms are even less frequent. Pouch procedures like the Hunt-Lawrence pouch are used with the Roux-en-Y procedure to augment the neogastrium′s reservoir capacity and to slow down the rapid emptying of food in the small gut, as both functions are important. Food transit through the pouch follows a linear decreasing function and is significantly slower compared to the exponential passage of oesophagojejunostomy, although both patterns remain still significantly accelerated compared to the physiological ranges of gastric emptying.[40],[41],[42] Now it is known that the beneficial effects of a pouch become apparent after a considerable period of time and the real assessment of its benefit must be done after a long follow-up.[43],[44] A randomised controlled trial has shown that a short pouch is more effective than a long pouch in maintaining nutrition and in preventing reflux symptoms.[45] Interposition of jejunal loop between the oesophagus and duodenum, although technically more demanding, restores the duodenal continuity, which maximizes absorption and helps in restoring nutrition. Although preservation of the duodenal passage is the more physiological approach to the restoration of the continuity of the digestive tract, surprisingly, the expected impact of the duodenal passage on symptoms, nutrition and outcome could not be ascertained by most of the studies, thereby negating the additional operative effort of jejunum interposition. Two randomised controlled trials have compared the outcome after jejunal interposition and after jejunal interposition with pouch formation; statistically proven benefits for pouch reconstruction could not be demonstrated by either study. Perhaps the reason for failure of the physiological superiority of preservation of the duodenal passage not getting translated into clinical benefit lies in the dennervation of the jejunal interposition. This has given rise to using the enervated jejunal loop for reconstruction.[46],[47] Similarly, the pylorus, pyloric branch of the vagus nerve and the lower oesophageal sphincter are being saved in modified surgical procedures ("nearly total gastrectomy" or "function-preserving gastrectomy"), wherever oncologically feasible, in an attempt to improve the motility of the reconstructed digestive tract.[48],[49],[50],[51],[52] The technical surgical problems of total gastrectomy having largely been solved, the question of quality of life must increasingly determine the choice of treatment. Clinicians now realize that malnutrition is not an inevitable consequence of total gastrectomy and can be prevented by an adequate calorie intake as a close relationship between dietary intake and postoperative nutritional parameters has been observed. In gastrectomized patients a strict nutritional follow-up can ensure an adequate dietary intake.[53] Most authors agree that maintenance of nutritional status and quality of life is similar after partial/subtotal and total gastrectomy, hence total gastrectomy, when clinically indicated, can be safely done without excessive concern about postoperative nutrition.[54],[55],[56] A randomised controlled trial has shown that patients who undergo subtotal gastrectomy have a better outcome during the first postoperative year, but patients given a gastric substitute after gastrectomy improve with the passage of time and have an even better outcome in the long run.[57] Only one prospectively randomised trial has compared various techniques of reconstruction after partial gastrectomy, and it favoured Roux en Y as the technique of choice when compared with Billroth I and Billroth II techniques of reconstruction.[58] Patients who have undergone total gastrectomy enjoy a good quality of life and most of them return to the preoperative lifestyle in 18 months. The global health status is not negatively influenced by D2 lymphadenectomy and extended gastrectomy.[59] Patients with splenectomy are more affected by treatment than patients without splenectomy.[60] As a palliative measure, gastro-jejunostomy and total gastrectomy performed with P2 or P3 peritoneal dissemination have no beneficial effect on the prolongation of survival or improvement of QOL of patients with gastric cancer.[61] As in palliation of Carcinoma oesophagus, self-expanding metal stents are a safe and efficacious method for palliating malignant gastric outlet obstruction, which has got a scale to grade its severity: gastric outlet obstruction scoring system.[62] Gall bladder surgery Gallstone disease has a profoundly negative impact on QOL, especially in symptomatic patients with a history of biliary colic attacks and/or the complications of the disease. Although the condition is not equally distressing for the asymptomatic group of patients without such a history, uncomplicated laparoscopic cholecystectomy (LC) improves QOL significantly in both groups. Gallstone patients with lower GIQLI scores are more likely to benefit from LC.[63] The occurrence of the much dreaded bile duct injury (BDI) has a great negative impact (P<0.05) on the patient′s physical and mental QOL. Despite excellent functional outcome after repair, the duration of the treatment of BDI is independently prognostic for a worse mental QOL.[64] Another study of QOL after BDI suggests that in spite of normal physical and social domains (comparable to those of control patients), the psychological dimension of decreased QOL assessment may be attributable to the prolonged, complicated, and unexpected nature of these injuries.[65] Pancreatic surgery GIQLI and the specific pancreatic module of EORTC are commonly used for assessing QOL in pancreatic patients. In patients with periampullary tumours, GIQLI has been divided into four subscales, measuring physical well-being, mental well-being, digestion and defecation. These subscales provide insight into the different problems affecting the patient.[66] Surgery is an excellent option for patients with chronic pancreatitis. Post-operatively, patients show significant (P<0.005) improvements in all aspects of the QOL survey. In addition, narcotic and alcohol use is significantly decreased.[67] Research workers have demonstrated that as a group, patients who survive pancreaticoduodenectomy have near-normal QOL scores. Many patients report weight loss and symptoms consistent with pancreatic exocrine and endocrine insufficiency, but most patients have QOL scores comparable to those of control patients and can function independently in daily activities.[68],[69] An important study has shown that general nutritional status, outcome and QOL are same in the pancreatico-gastrostomy and pancreatico-jejunostomy groups.[70] Whenever feasible, Beger′s duodenum-preserving pancreatic head resection should be done as in terms of QOL, it gives better long-term results than classical Whipple pancreatoduodenectomy.[71] In elderly inoperable patients, endotherapy in the form of an endoprosthesis to treat jaundice improves the patient′s QOL. However, surgical palliative bypass procedures retain their importance in underdeveloped countries where endoscopic stenting may not be available to large sections of the population.[72] Just like in every other disease, pancreatic patients are the best source to describe and assess their QOL.[73] Liver Surgery Liver transplantation is believed to improve QOL. As the number of liver transplantations performed around the world and the survival rates increase, attention is turning to the broad impact this procedure has on patients′ QOL. There exists a small body of literature that examines the global effects of liver transplantation on QOL.[74],[75] Knowledge of the factors related to QOL outcome after liver transplantation is important because it might allow development of new interventions that may have an impact on future allocation decisions. Establishment of a standard database has been suggested so that a validated instrument will be available to compare QOL results from all the liver transplantation programs. Similarly, hepatic resection results in significant enhancement of QOL in patients with Hepatocellular Carcinoma (HCC). Recurrence is the main factor leading to deterioration in QOL over time after resection of HCC.[76] COLO-RECTAL SURGERY Surgery of benign anorectal disorders Very few studies have evaluated the QOL in benign anorectal disorders. Sailer et al used GIQLI to establish baseline values of QOL for different benign anorectal disorders like haemorrhoids, anal fissure, fistula in ano, severe constipation, fecal incontinence, symptomatic rectocele, peri-anal abscess and peri-anal thrombosis. They found that the subgroups of patients with painful fissures, severe constipation and fecal incontinence had a significantly poorer QOL than age-matched healthy individuals.[77] As expected, the impact of incontinence on QOL is very significant and the degree of incontinence (evaluated by the Wexner score and Fecal Incontinence Severity Index) correlates with poorer QOL.[78],[79] Cut-off values of these scores can be used to define significantly poor QOL and can be used as decision-making tools for deciding to repair the sphinctor. Surgery has been shown to improve initially low QOL and symptomatic complaints in patients with dyschezia and a rectal static disorder like rectoceles, independently of anatomic repair.[80] Similarly, dynamic anal graciloplasty and tran-anal electrostimulation, both improve QOL in incontinent patients, as does colectomy for patients with chronic intractable constipation.[81],[82],[83] Ileo Anal Pouch Procedure (IAPP) Many Inflammatory Bowel Disease (IBD) Questionnaires work as reliable and valid measures of the QOL of IBD patients. QOL assessment is an invaluable tool in determining the overall functional outcome after ileal pouch-anal anastomosis (IPAA). The Cleveland Global Quality of Life score or Fazio score, a novel quality-of-life instrument has been specifically designed for patients with ileal pouches. Many studies have shown that QOL improves significantly after IPAA in patients with Ulcerative Colitis (UC) and is equal to that in normal individuals, if postoperative complications are either prevented or under control.[84] As expected, frequency of bowel movements and degree of continence are the key to QOL in these patients, while night-time stool frequency influences QOL the most.[85] Most patients suffer dietary restrictions, forcing them to adopt a fixed dietary regimen. Composition of diet and timing of intake are important determinants of QOL after ileal pouch formation. Patients with familial adenomatous polyposis and those with a history of pouchitis had poorer QOL scores than ulcerative colitis patients without a background of pouchitis. These differences do not correlate with poorer pouch function, highlighting the influence of non-pouch-related factors in QOL after ileal pouch formation.[86] Functional outcome after IPAA is not as good in older patients, however, appropriate case selection and proper preoperative counselling, vis-à-vis expectations from the surgery confers acceptable function and QOL on patients of all ages.[87] Functional outcome of major revisional surgery for symptomatic retained rectal stump after restorative proctocolectomy is worse than the outcome following first-time restorative proctocolectomy with anastomosis constructed at the anal level.[88] A panproctocolectomy and permanent ileostomy improves the QOL of those suffering from ulcerative colitis. It has been shown that despite the fact that these patients underwent major surgery and have a permanent stoma, their QOL is very similar to that of the general population.[89] The functional outcome and QOL of laparoscopic-assisted ileal pouch-anal anastomosis is not different from conventional ileal pouch-anal anastomosis.[90] The trade-off of neoplasia control for better function represented by a stapled IPAA is still controversial in patients with familial adenomatous polyposis (FAP). Fazio et al compared outcomes after mucosectomy and hand-sewn ileal pouch-anal anastomosis with those after stapled ileal pouch-anal anastomosis in 119 patients with familial adenomatous polyposis who underwent surgery. Patients with stapled anastomosis had better outcomes, vis-à-vis incontinence, daytime and night-time seepage, pad usage, and avoidance of ileostomy. They concluded that familial adenomatous polyposis patients with stapled ileal pouch-anal anastomosis have better functional outcome and can avoid temporary diversion, but this advice should be balanced against a 28% incidence of adenomas in the anal transitional zone.[91] UC patients after IAPP, when compared with FAP patients are more likely to develop pouchitis; despite this both patient groups enjoy a similarly good functional status and QOL.[92] Crohn′s Disease When analysing the QOL for Crohn′s Disease (CD), the patients′ main worries are "having an ostomy bag" followed by "uncertain nature of the disease," "energy level" and finally "having surgery." Use of tobacco, hospitalisation, and use of corticoids have a negative impact on QOL. Conversely, the use of immunosuppressors is associated with a better QOL.[93] Colorectal oncosurgery Popularity of sphincter-saving resections has resulted in concomitant drastic reduction in extirpations of the rectum with permanent colostomy. This development is paralleled by increasing research into postoperative QOL in colorectal cancer. The Medical Outcomes Study Short Form 36 (SF-36), and the European Organization for the Research and Treatment of Cancer QLQ-C30 and QLQ-CR38 QOL questionnaires are commonly used to assess QOL after colorectal cancer surgery. A similar understanding of the importance of QOL is fuelling the current resurgence of transanal excision with adjuvant therapy. Anterior resection Anterior resection and non-stoma patients, despite suffering micturition and defecation problems, have better QOL scores than abdominoperineal extirpation and permanent stoma patients. Comparisons between abdominoperineal extirpation and anterior resection patients should also consider the effect of temporary stomas. QOL scores may be dynamic, improvements in QOL scores over time may be explained by reversal of temporary stomas or physiologic adaptation, supporting the use of longitudinal QOL assessment in these patients.[94],[95],[96] However, the patient has to be informed preoperatively about possible side-effects associated with surgical procedures such as coloanal anastomosis or neosphincter reconstruction, to avoid severe psychological difficulties later on.[97] The women patients are more sensitive to the presence of a stoma, and it affects their QOL much more than the male patients.[98],[99] When straight and colonic pouch anastomoses after rectal excision for cancer are compared, there is an advantage for the pouch group regarding frequency, urgency and incontinence but surprisingly, this observed difference in clinical bowel function was not reflected in a better QOL score as studied with Nottingham Health Profile.[100] Sphincter-sparing surgery after preoperative RT seems to be feasible in routine practice, in a significant proportion of low rectal cancers without compromising the oncologic results.[101] But many patients with advanced rectal cancers who require external beam radiation therapy, extensive pelvic surgery, and intraoperative radiation therapy report unfavourable functional and quality-of-life outcomes after sphincter preservation. In this setting patients being considered for coloanal anastomosis or very low anterior resection may be better served by permanent diversion.[102] This shows that a very ambitious preservation of the sphincter does not automatically lead to good QOL. Formation of a permanent stoma affects aspects of religious worship and adversely affects QOL in Muslim patients. Preoperative counselling, the informed consent process, and counselling with local religious authorities is recommended in such situations.[103] Extensive surgery A large proportion of patients suffered various urinary tract problems due to extended lymphadenectomy, giving rise to preservation of inferior hypogastric nerve plexus and the advent of autonomic nerve-sparing surgery.[104] Pelvic exenteration (PE), the most radical operation for rectal cancer, is indicated in a small proportion of patients with extensive primary or locally recurrent rectal cancer, when the disease remains confined to the pelvis for a prolonged period. PE carries a high risk of perioperative morbidity and mortality, and has profound functional, psychological, and psychosexual implications for patients. Careful preoperative counselling regarding surgical risks and the impact of PE on body function and image is indispensable; the patient′s consent must be truly informed.[105],[106] Patients after major exenterations are concerned about stomas and poor body image. In a prospective longitudinal study, patients with two ostomies reported a significantly lower QOL (P=0.008) and poorer body image (P=0.002) than patients with no ostomy.[107] Thus, organ reconstruction should be performed whenever possible in patients with pelvic exenterations, but fear of reducing the patient′s QOL should not be a major contraindication when surgery with urinary diversion is warranted to obtain curative resection.[108] Recurrence of rectal cancer Tumour recurrence is the decisive factor determining postoperative QOL and has a profound effect on QOL, affecting most measurable dimensions. Treatment of recurrent cancer should not only be directed at the physical aspect of the disease, but also at its psychological and social aspects.[109] In appropriately selected cases, aggressive surgical therapy produces significant disease-free survival in patients with recurrent rectal cancer. Salvage surgery for recurrence after local excision of rectal cancers may not provide results equivalent to those of initial radical treatment and its wisdom has been questioned.[110],[111] In cases of inoperable rectal cancer recurrence, the placement of self-expanding metal stents is technically feasible and safe, avoids a permanent colostomy resulting in preservation of QOL.[112] QOL, SURVIVAL AND OTHER ISSUES IN RECTAL CANCER Preoperative QOL is a strong independent predictor of survival at 1 year.[99],[113] Patients with colorectal cancer, like any other patients, want independence in activities of daily living and this is reflected in their QOL as well.[114],[115] QOL of patients who have a pelvic pouch for colitis-associated neoplasia is excellent and the same as that of patients who have a pouch for failure of medical therapy of UC.[116] LAPAROSCOPIC-ASSISTED COLECTOMY Laparoscopic-assisted colectomy (LAC) has emerged as the preferred minimally invasive surgical strategy for diseases of the colon but a multicentre randomised controlled trial by Clinical Outcomes of Surgical Therapy (COST) Study Group has shown that LAC confers only minimal short-term QOL benefits for colon cancer compared with standard open colectomy. They cautioned that until ongoing trials establish that LAC is as effective as open colectomy in preventing recurrence and death from colon cancer, this procedure should not be offered to patients with colon cancer.[117] GASTROINTESTINAL (GI) CANCERS PER SE With better and earlier detection and treatment, GI cancer is getting transformed from an acute life-threatening disease to a chronic life-threatening disease. In this scenario, assessment of QOL assumes even greater importance. And that is the reason more and more researchers are accepting survival and QOL as two different end points in GI cancers. "When cure is elusive, it is time to start treating the patient; not the tumour."[118] It is crucial that newer loco-regional treatments like cryotherapy/microwave coagulation necrosis for hepatocellular carcinoma and chemotherapeutic agents are incorporated in prospective randomised trials along with QOL measures to assess their efficacy. Assessment of QOL in cancer patients is not easy but this challenge is increasingly being successfully tackled. WHAT IS THE FUTURE OF QOL STUDIES? QOL studies were in the past criticized on the grounds that QOL variables are ′soft′ and subjective therefore cannot be measured accurately (measuring the unmeasurable?); they provide data which are neither interpretable nor clinically meaningful and that they are too intrusive to the patient making them unacceptable. But the tide of accumulated evidence in favour of QOL studies, over the years, has washed away these criticisms like words written on a sandy beach. The questions ′What is it?′, ′How is it measured?′ and ′How can the information be used?′ are now better understood than a few years ago; and all the qualms about QOL studies have been put to rest.[119] Assessment of HRQOL has been the missing measurement in healthcare but has now ′come of age′ and will be incorporated increasingly into the decisions of clinicians and policy-makers. However, QOL measurement in surgery is currently done mainly for research purposes, and unless it finds a beneficial place in routine clinical practice, it is likely to remain a philosophical exercise. Developments in this field will lead to widespread use of QOL measurements in all surgical disciplines as part of routine clinical practice. HRQOL as a prediction of treatment response is another interesting option, even though more work must be done in this area. Another important area of growth is incorporation of QOL in both medical school and continuing education for clinicians. Study of QOL is certainly much more than a fashion, it is a new science, an idea whose time has come. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04085f1.jpg] |
| |||||||||

{kind=link}