 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
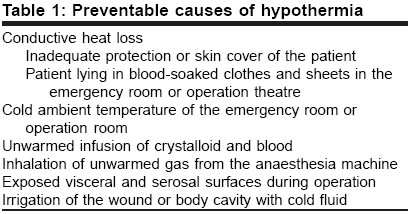
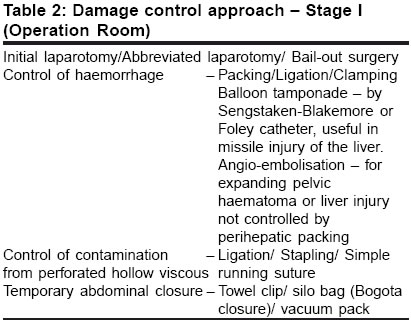
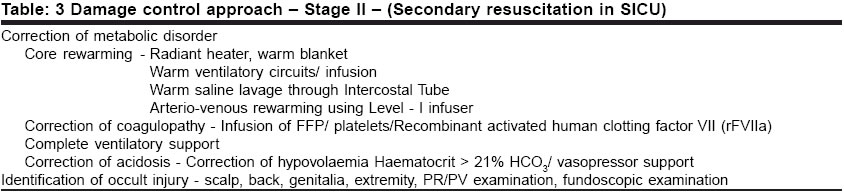
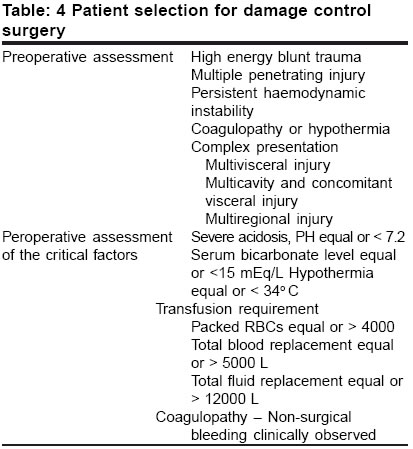
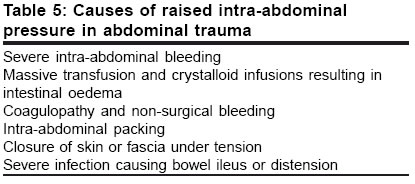
Indian Journal of Surgery, Vol. 66, No. 6, November-December, 2004, pp. 336-340 Review Article A logical approach to trauma - Damage control surgery Ghosh Shibajyoti, Banerjee Gargi, Banerjee Susma, Chakrabarti DK Department of Surgery, R. G. Kar Medical College, West Bengal Code Number: is04086 ABSTRACT Trauma is the major cause of death worldwide. Survival of the major trauma victims can be improved by the principles of damage control surgery. The vicious cycle of trauma triad, namely, hypothermia, coagulopathy and acidosis should be intercepted by the quick abbreviated laparotomy and subsequently physiological imbalance is corrected by secondary resuscitation in the surgical intensive care unit. Definite repair can be taken later on. Abdominal compartment syndrome is the most formidable complication. Multidisciplinary team approach is needed to alleviate the physical and psychological trauma of the patient. KEY WORDS: Damage control surgery, trauma triad, hypothermia, coagulopathy, acidosis, abdominal compartment syndrome. Damage control surgery following trauma is one of the major advances in surgical practice in the last 20 years. The principles of damage control surgery were slow to be accepted worldwide because it defied the traditional surgical teaching that, the first chance of any surgical intervention is the best chance for any definitive repair or reconstruction, with good result. HISTORICAL PERSPECTIVE OF DAMAGE CONTROL SURGERY In the seventh and eighth decades of the last century, huge developments in science and technology were also reflected in the operation theatre and intensive care units. There was better understanding of body physiology supported by excellent equipment for intraoperative and postoperative monitoring of the patient along with adequate blood banks. Surgeons at that time took up the challenge of trauma surgery more aggressively for complete repair of complex injuries at the first chance. The patients could survive the initial onslaught but soon they succumbed to a new kind of clinical situation. Conditions like shock lung syndrome or ARDS (Adult Respiratory Distress Syndrome), SIRS (Systemic Inflammatory Response Syndrome), MODS (Multi Organ Dysfunction Syndrome), MOF (Multiple Organ Failure) were recognized and ultimately, the majority of these patients died early in the postoperative period. Trauma surgeons began to introspect and tried to find out an alternative approach of this hugely expensive and frustrating exercise. Thus the concept of damage control surgery emerged almost simultaneously all over the world towards the end of 1980.[1],[2] It was found that the cause of death in these trauma victims was not due to failure to complete the initial operation. The patients died because of the metabolic derangement or physiological alteration in the body following severe exsanguinating polytrauma, characterized as the trauma triad of death. These were hypothermia, coagulopathy and acidosis.[3] DAMAGE CONTROL STRATEGY The conventional sequence of the management of trauma surgery was to bring the patient to the operating room after initial resuscitation and then to operate for complete repair of the injuries. Even patients with multiple complex injuries were operated more aggressively over a prolonged period of time for definitive primary repair. Subsequently, these patients were sent to the intensive care unit where a good number of the patients succumbed due to metabolic derangement of the body. The principles of damage control surgery replaced this sequence.[4] At the first phase of damage control strategy, only abbreviated laparotomy was done for lifesaving measures, then the patient was sent to the surgical intensive care unit (SICU) for the correction of the metabolic disorder. Following satisfactory correction the patient was once again taken to the operation room for definitive repair and sent back to SICU for further convalescence. TRAUMA TRIAD The policy of damage control surgery was developed on the realization that most of the severely exsanguinating and polytrauma patients died from a triad of coagulopathy, hypothermia and metabolic acidosis. Once metabolic failure has become established it is extremely difficult to control haemorrhage and correct the physiological derangements. Hypothermia - It is the inevitable sequence of severe exsanguinating injury and subsequent massive resuscitative effort.[5] Severe haemorrhage causing hypovolaemia leads to tissue hypoperfusion in the body. This means diminished oxygen delivery at the cellular level and reduced heat generation. Clinically, hypothermia is important if the body temperature drops down to less than 97° F or (36°C) persistently for more than 4 hours.[6] Hypothermia can lead to cardiac arrhythmias, decreased cardiac output, increased systemic vascular resistance, left shift of oxygen-haemoglobin dissociation curve, and can induce coagulopathy by inhibition of clotting cascade reactions.[7],[8] The immunological surveillance system is also impaired at a low temperature and this could play a crucial role in the survival of the patient. The surgeon should be aware of these consequences and should take every measure to prevent further exaggeration of hypothermia, which is easily preventable. Hypothermia is aggravated by heat loss either by conduction or convection due to environmental factors and common practices followed in the emergency room or operation theatre [Table - 1]. Coagulopathy - Every aspect of the normal clotting mechanism is affected in a cold acidotic exsanguinating patient. At a low temperature all the clotting cascade reactions are inhibited producing decreased amount of clotting factors. Also, the balance between thromboxane and prostacycline is affected in the hypothermic state, resulting in platelet dysfunction. Severe injury and certain injury complexes like head injury had shown to increase fibrinolysis. Thus, coagulopathy occurs due to hypothermia, platelet dysfunction at low temperature, activation of the fibrinolytic system and haemodilution following massive resuscitation. Hypothermia and haemodilution have an additive effect on coagulopathy than either factor alone.[9] Different laboratory parameters of the coagulation profile, like prothrombine time, partial prothrombine time, fibrinogen level, and lactic acid level, are not very much predictive of the onset of a severe coagulopathic state in a cold, exsanguinating patient. In the intraoperative period, the clinical judgment of the senior surgeon to identify coagulopathy should be considered for damage control measures.[4],[10] Acidosis - Anaerobic cellular metabolism starts when the shock stage or hypoperfusion is prolonged, producing lactic acidosis. Acidosis is further increased by massive transfusion, use of vasopressor drugs, aortic cross-clamping, and impaired myocardial performance. Consequently, the normal clotting mechanism is altered in the acid medium of the body. It is clearly evident that a complex relationship exists between these three factors and the presence of one factor accentuates the other factor leading to progressive metabolic failure and death. To break this vicious triad of death, a systemic three-phase approach was designed as a damage control approach. DAMAGE CONTROL APPROACH: STAGE I Primary resuscitation should start from the field and be continued to the operation room. The first stage consists of initial laparotomy which is also known as abbreviated laparotomy or bail-out surgery. Lifesaving procedures [Table - 2] are performed very rapidly and the operation is abbreviated by temporarily closing the abdomen. Control of haemorrhage is the top priority by quickly clamping and ligating the major vessels. Perihepatic packing is most important for controlling bleeding in grossly lacerated liver injury or if the bleeding cannot be controlled by the conventional methods. Optimum compression should be done from both sides, superior and inferior surface of the liver, to achieve haemostasis. The drawback of this method is that underpacking may fail to stop bleeding whereas overpacking may increase intra-abdominal pressure. Intra-cavitary bleeding of the liver from missile tracts can be controlled by balloon tamponade. Hollow viscous injuries are dealt with simple closures to prevent contamination. No attempt is made for complex repair at this stage. Thorough irrigation of the body cavities with warm isotonic solution should be done and quick temporary closure of the abdomen can be achieved by the help of towel clips.[11] In case of massive bowel oedema and distension, direct closure of the abdomen may lead to abdominal compartment syndrome. In such a situation silo bag closure[12] or vacuum pack[13] closure is useful to prevent rise in the intra-abdominal pressure. DAMAGE CONTROL APPROACH: STAGE II (SICU) The second phase of damage control service begins in the SICU where the resuscitation team tries hard to correct the metabolic disorder. Rewarming the patient is a high priority as coagulopathy and acidosis can only be corrected and maintained when the body temperature returns to normal. Simple measures as well as complex invasive procedures may need to be done for core rewarming of the body temperature [Table - 3]. As the resuscitation progresses, further inspections are made to identify occult injuries which are missed at the initial survey. The scalp, back, genitalias, and extremities are the common sites for missed injuries. Twenty-four to 48 hours are needed to correct the metabolic derangement. When the patient is adequately warm and the coagulation profile is satisfactory, reverting back to the normal serum lactate level is considered as the end point of secondary resuscitation.[14] DAMAGE CONTROL APPROACH: STAGE III (PLANNED REOPERATION) The timing of planned reoperation is critical. There is usually a window period, 36 to 48 hours after the trauma, between the correction of metabolic disorder and the onset of SIRS and MOF.[15] In this phase definitive procedures are undertaken. Perihepatic packing or other packing is removed and small bleeding vessels are controlled. A thorough exploration is made for any hidden injuries. Restoration of gastrointestinal continuity and vascular repair are done. Provision for enteral feeding by jejunostomy or gastrostomy as appropriate is made. A thorough washout of the abdominal cavity with copious amount of warm isotonic fluid is done before primary definite closure is attempted. The patient is then shifted to SICU for further convalescence. Other than planned reoperation the patient may sometimes need early unplanned reoperation for ongoing haemorrhage, abdominal compartment syndrome or peritonitis. PATIENT SELECTION FOR DAMAGE CONTROL MEASURES [Table - 4] Only a small percentage of trauma patients require damage control measures[10] and early identification of these cases produces optimal results. Certain conditions and complexes when assessed preoperatively can alert the surgeon about the possible damage control intervention.[5] Peroperative assessment of some critical factors in unassuming cases also calls for damage control application. Asensio et al[16] recommended certain intra-operative parameters as a guideline for instituting damage control. They suggested damage control intervention before reaching the upper limits of these parameters, which include pH less than or equal to 7.2, serum bicarbonate level less than or equal to 15 mEq/L, core temperature less than or equal to 34°C, transfusion volume of packed RBCs more than or equal to 4000 ml, total blood replacement more than or equal to 5000 ml, or total fluid replacement more than or equal to 12000 ml. The success of damage control surgery depends on a disciplined approach, which includes proper decisions, rapid control, and rapid termination of the operation. COMPLICATIONS OF DAMAGE CONTROL SURGERY Abdominal compartment syndrome The abdominal compartment syndrome is a lethal complication of severe abdominal trauma as well as abbreviated laparotomy. Unless recognized early this inflicts the other systems of the body leading to multi-organ failure. Causes of raised intra-abdominal pressure in abdominal trauma are listed in [Table - 5]. When the abdominal pressure rises to more than 25 cm of H2O, significant cardiovascular, respiratory, renal and cerebral dysfunction occurs. There is compression of the inferior vena cava and diminished cardiac return of the blood due to abdominal hypertension. Cardiac output is reduced while central venous pressure (CVP), pulmonary artery wedge pressure and systemic vascular resistance are increased. Respiratory parameters are altered because the diaphragmatic movement is restricted resulting in increased intrathoracic and peak airway pressure. As a result of this, intractable hypercapnia can occur due to poor compliance of the lungs. Oliguria and anuria can be precipitated by the compression of the renal vein and renal parenchyma. The central nervous system is also affected as intracranial pressure is increased due to increased CVP preventing adequate venous drainage from the brain. The abdominal compartment syndrome should be suspected in any patient having a period of profound shock with multiple trauma. Clinical features are abdominal distension, increased airway pressure, difficulty in ventilation, and oliguria or anuria. The diagnosis can be confirmed by measuring the intra-abdominal pressure. This can be done by simple indirect method, either through a 3-way Foley catheter in the bladder or Ryle′s tube in the stomach, attached to a water column manometer. Normal intra-abdominal pressure is zero cm of H2O or less. Pressure over 35 cm of H2O (Grade IV)[17] is diagnostic. Management -Abdominal decompression is immediately indicated. Laparotomy and methods for temporary abdominal closure by towel clip, silo or zipper laparostomy should be considered. However, sudden decompression can produce some deleterious effects. As the compressed abdomino-pelvic veins are released, the effective cardiac preload is reduced and a bolus of acid, potassium, and other by-products of anaerobic metabolism are washed into the systemic circulation. This may develop cardiac asystole, known as reperfusion syndrome.[18],[19] GENERAL COMPLICATIONS These patients are basically very ill patients and they tend to suffer from the same kind of complications as other critically ill surgical patients. Wound sepsis and wound dehiscence are more common because of very high contamination. Risk of fistula formation is increased with pancreatic injury, proximal bowel injury and bowel exposed to air following dehiscence. ICU-related infections like central line infection, suppurative thrombophlebitis, sinusitis, pneumonia are not uncommon. Prophylactic heparin is indicated in high-risk patients like spinal cord injury, pelvic or lower extremity fracture when coagulopathy and bleeding is controlled. Special mattresses and proper nursing care are needed to prevent skin complications. Psychological support and regular communication with the relatives of the patients are the other important aspects of this challenging surgical management. CONCLUSION Damage control surgery represents an important landmark in the historical spectrum of trauma resuscitation. In trauma surgery, prolonging the initial operation can lead to disastrous results. Curtailing the operation does not mean abandoning but it gives a chance to survive in an otherwise hopeless situation. It is difficult to learn when to stop and can be learned only from experience. The management of this complex problem requires a multidisciplinary team approach with patient counselling and communication with the family. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04086t4.jpg] [is04086t3.jpg] [is04086t1.jpg] [is04086t5.jpg] [is04086t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}