 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 6, November-December, 2004, pp. 341-346 Original Article Role of helicobacter pylori in functional dyspepsia Shrivastava UpendraK, Gupta Aman, Gupta Arun, Bhatia Arati Departments of Surgery, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi - 110095 Code Number: is04087 ABSTRACT BACKGROUND: The association of Helicobacter pylori with functional dyspepsia is widely reported, but it remains unclear whether H. pylori infection actually causes symptoms or is just an associated finding.AIMS: This study was conducted to determine the role of H. pylori in causing symptoms of functional dyspepsia and to observe any improvement in symptoms after eradication of H. pylori. SETTING AND DESIGN: This study was conducted in a prospective, randomised double-blind manner at the Surgery Department of our institution. MATERIALS AND METHODS: Eighty patients with functional dyspepsia were randomly distributed into two groups to receive eradication or placebo therapy after taking biopsies for H. pylori. Symptom evaluation was done at baseline, at one and at three months to notice any improvement. STATISTICAL ANALYSIS: Changes in the dyspepsia score were compared using ANOVA test at baseline, one and at three months to compare the improvement in symptoms. RESULTS: Approximately two-thirds of patients with functional dyspepsia are infected with H. pylori. Significant long-term improvement was observed after eradication in H. pylori infected patients. No significant improvement was seen with placebo therapy. CONCLUSION: H. pylori plays a significant role in causing symptoms of functional dyspepsia. Treatment with triple drug regimen brings a significant long-term improvement in the symptoms. KEY WORDS: Helicobacter pylori, functional dyspepsia INTRODUCTION Dyspepsia is defined as upper abdominal or retrosternal pain or discomfort referable to the proximal alimentary tract. Dyspepsia is a major health problem. The prevalence of dyspepsia ranges from 20%-30% in the general population.[1] It may be associated with peptic ulcer disease, gastroesophageal reflux disease, and gastric cancer. However, the most frequent type is functional dyspepsia which is defined as persistent or recurrent upper abdominal discomfort in whom a reasonable clinical evaluation has failed to reveal a definite cause of the symptoms.[2] The pathogenesis of functional dyspepsia is unknown. Many pathogenic mechanisms have been proposed, like disturbance in gastric acid secretion, disordered gastric motility, abnormalities of electrical control activity, abnormalities of perception, psychological disturbances, environmental factors and Helicobacter pylori (H. pylori).[3] Although the role of H. pylori has been documented in the pathogenesis of peptic ulcer, its role in causing symptoms of functional dyspepsia is not clear. The reported prevalence of H. pylori in patients with functional dyspepsia ranges from 39%[4] to 87%,[5] but it remains unclear whether H. pylori infection actually causes symptoms or is just an associated finding. Many trials evaluating the role of H. pylori in functional dyspepsia and the efficacy of H. pylori eradication treatment on the symptomatology of functional dyspepsia have been published in the past, but most of these have given conflicting results. This prospective, randomised, double-blind study was undertaken to determine the role of H. pylori in causing symptoms of functional dyspepsia and to see if the eradication of H. pylori infection could bring some improvement in the symptomatology. MATERIALS AND METHODS The study was conducted over a period of 1½ years from July 2001 to December 2002. The study protocol was approved by the review board of our institute for ethical research. Written informed consent was obtained from all patients. A total of 80 patients presenting with symptoms of dyspepsia were enrolled and investigated to rule out any organic disorder. Dyspepsia was defined as upper abdominal pain or discomfort of more than three months duration associated with any of the following:
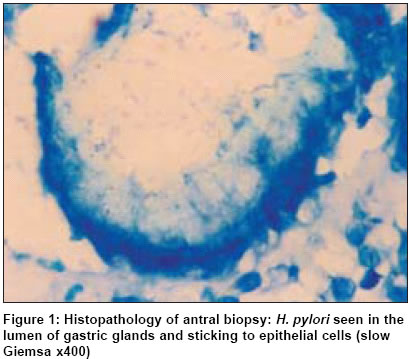
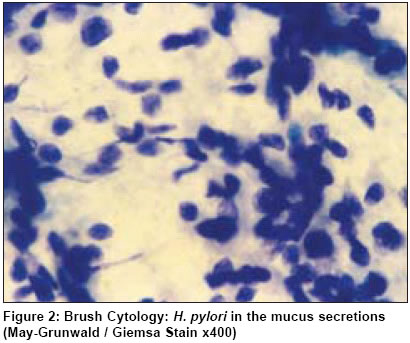
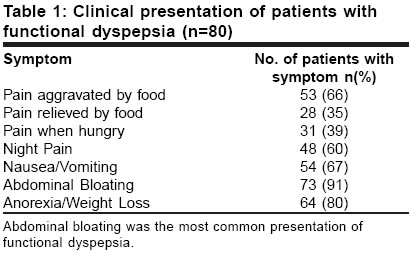
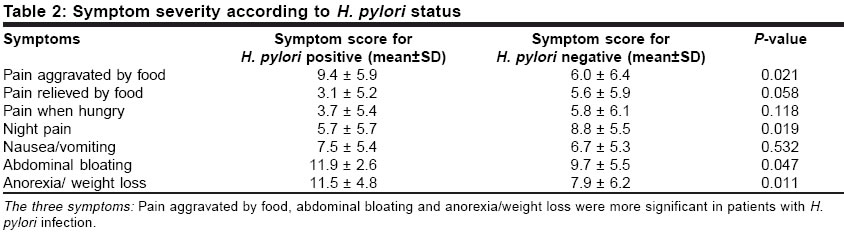
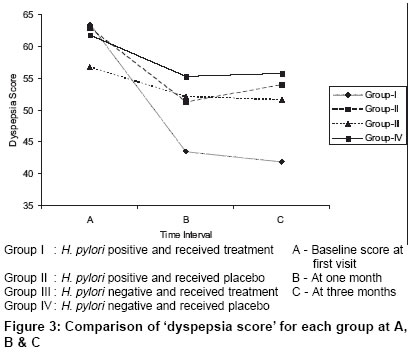
Exclusion Criteria Patients having any organic disease, history of alcoholism, use of steroids/NSAIDS, pregnant and lactating females were excluded from the study. Study Design Ultrasound examination of whole abdomen and upper GI endoscopy were carried out on all patients to rule out the presence of any underlying organic disorder. All the patients were interviewed personally by an investigator and detailed symptomatology of all the patients was recorded. The interviewer was unaware of the H. pylori status and the treatment given to the patient. The symptoms were graded on the basis of frequency and severity using adjectival scale and visual analogue scale. The total score for each symptom was calculated by adding the score on each of the above two scales. The total dyspepsia score was calculated for each patient by adding the scores for individual symptoms. During upper GI endoscopy, three antral biopsy specimens and one brush cytology specimen were collected from each patient. After each endoscopy, endoscopes and biopsy forceps were sterilized with 2% gluteraldehyde for 30 minutes to prevent cross-infection among patients. The antral biopsy specimens were subjected to Rapid Urease Test, Gram Staining, Haematoxylin and Eosin Staining and Slow Giemsa Staining [Figure - 1]. The brush cytology specimens were tested for the presence of H. pylori by modified May-Grünwald / Giemsa Staining[6],[7] [Figure - 2]. All the cases were randomly distributed into two groups without knowing their H. pylori status. Randomisation was done by a random number technique using computer-generated random numbers. One group received treatment for H. pylori for one week consisting of Amoxycillin 750 mg, Clarithromycin 250 mg and Omeprazole 20 mg twice daily for 7 days (GI Kit, Biological E, Hyderabad). The other group received placebo therapy for one week. The placebo consisted of similar-looking capsules as the treatment drugs. Packets of drug treatment and placebo were sealed blindly in similar envelopes and coded. The codes were kept secret from the treating physician and the patient. The patients were clinically re-evaluated at one month and at three months after the completion of treatment to assess any improvement in symptoms by the same investigator who was not aware of the H. pylori status and the treatment received by the patient. The patients′ symptoms were again graded on both the adjectival and visual analogue scale. The total dyspepsia score was calculated for each patient. At the end of the study all the patients were distributed into 4 groups on the basis of their H. pylori status and whether they received drug treatment or placebo. Group I : H. pylori positive and received treatment A patient was regarded as H. pylori positive if one or more of the applied diagnostic methods were positive. A patient was considered to be H. pylori negative if all the applied methods were negative. Statistical Analysis Mean scores for all the symptoms and total dyspepsia score were compared in the H. pylori positive and H. pylori negative group using unpaired ′t′ test. Clinical presentation in terms of number of patients with each symptom in H. pylori positive and H. pylori negative group were compared using chi-square test. The groups were compared at baseline and at two consecutive visits for total dyspepsia score using hierarchal analysis of variance (ANOVA), and multiple comparisons were obtained using Tukey′s test at 5% level. P value <0.05 was considered as significant. RESULTS There were 51 male and 29 female patients (M : F - 1.8:1). Age ranged from 16 to 60 years (mean 35 years). All the groups were well balanced for baseline demographic features. A total of 65% of patients were positive and 35% were negative for H. pylori. Seventy-one per cent of the males and 55% of the females were positive for H. pylori. The difference was not statistically significant (P=0.118). In the younger age group (<30 years) only a small percentage of patients had H. pylori infection. Beyond the age of 30 years, more than 80% of the patients were found to be positive for H. pylori. Abdominal bloating was seen to be the most common presentation (91%) in all patients with functional dyspepsia [Table - 1]. The symptom scores for the three symptoms: pain aggravated by food, abdominal bloating and anorexia/weight loss, were significantly higher in patients with functional dyspepsia who were positive for H. pylori as compared to those who were negative [Table - 2]. There was no significant difference in the total dyspepsia score (63.1±11.2, CI=60.0±66.3 vs. 60.2±8.1, CI=57.1±63.4; P=0.227, DF=78) between the H. pylori positive group and the H. pylori negative group. The comparison of dyspepsia scores between the four groups at presentation and then at follow-up at one and at three months shows a noticeable difference between the four groups [Table - 3]. In Group I (H. pylori positive and received treatment), a significant difference (P<0.001, DF=3, 16) in the dyspepsia score is seen at presentation and follow-up. The dyspepsia score improved from 63.4±12.3 at presentation to 43.5±8.4 at one month and further improved to 41.9±8.3 at three months. There is some improvement in dyspeptic patients at one month with drug treatment even if they are negative for H. pylori. However, no further improvement is seen at three months follow-up. Improvement in dyspepsia score at one month is seen in both H. pylori positive and H. pylori negative patients even if they receive placebo therapy. However, follow-up at three months shows a rising trend of the dyspepsia score in all these patients [Figure - 3]. DISCUSSION The aetiology of functional dyspepsia remains elusive. The association of functional dyspepsia with H. pylori infection has been widely reported. However, whether the association is casual or causal, remains debatable. Several studies have assessed the epidemiological association between H. pylori infection and functional dyspepsia. In our study, 65% of the patients were positive and 35% were negative for H. pylori infection. These results are comparable to the reported prevalence of H. pylori in patients with functional dyspepsia.[8],[9] The maximum number of patients with functional dyspepsia was seen in the age group of 21-30 years (34%). As the age advanced, the percentage of patients with functional dyspepsia decreased. Interestingly, however, the number of patients with H. pylori infection was found to be more in the higher age groups. Similarly, other investigators have reported that although the prevalence of functional dyspepsia is greater in patients under 25 years of age, the prevalence of H. pylori infection increases with age.[3],[10],[11] The comparison of dyspepsia scores between the four groups at presentation and then at follow-up at one and at three months showed a noticeable difference between the four groups. It was observed that patients who were positive for H. pylori and were given drug therapy showed a statistically significant improvement in the dyspepsia score at the end of one month, which persisted even at the end of three months. Placebo also resulted in transient improvement in symptoms at one month but deterioration was seen at three months. Earlier studies regarding the role of H. pylori in functional dyspepsia have given conflicting results. Many studies have shown good symptomatic response after anti-H. pylori treatment in patients with functional dyspepsia[12],[13],[14] whereas others have not observed a positive effect of anti-H. pylori treatment on symptoms of functional dyspepsia.[15],[16],[17] The results of the present study are in favour of an aetiological role of H. pylori in patients with functional dyspepsia. H. pylori was found in 65% of the patients with functional dyspepsia. Significant improvement in symptoms was seen only after eradication of H. pylori. The symptomatic response in these patients persisted even at three months after the start of therapy. Previous studies have also demonstrated that a short-term symptomatic response may be achieved without the eradication of H. pylori but with eradication of H. pylori the symptomatic response lasts for up to one year.[18] In patients with H. pylori negative functional dyspepsia a certain degree of symptomatic improvement was observed, although it was not statistically significant and no further improvement was seen at three months. The probable cause of such transient improvement may be acid suppression by Omeprazole or psychological support by placebo. On comparison of the symptomatology of all patients, it was seen that pain aggravated by food, weight loss and abdominal bloating were more significant in patients with H. pylori than those without H. pylori infection. Similar to our study, Viara et al (1992) have shown a significant association between H. pylori infection and postprandial bloating.[19] Werdmuller et al have also shown that weight loss is significantly more common in the H. pylori infected patients.[20] On the other hand, Sarnelli et al demonstrated no difference in the clinical presentation of patients with or without H. pylori infection.[21] Recent reviews have highlighted the methodological problems in most of the therapeutic trials of anti-H. pylori treatment in patients with functional dyspepsia. We have tried to eliminate most of the problems of the earlier studies.[22],[23] The present study was a prospective randomised double-blind trial. A strict definition of functional dyspepsia was used.[2] Patients with predominant symptoms of gastroesophageal reflux disease (e.g. heart burn) and irritable bowel syndrome (e.g., lower abdominal cramps or altered bowel habits) were not included in the study. The adjectival scale was used to grade the symptoms before and after treatment in addition to subjective assessment by the visual analogue scale. The adjectival scale has been demonstrated to be a satisfactory scale and it fulfils the properpties of reproducibility, responsiveness and validity.[22],[23] H. pylori infection was treated with a high-efficacy eradication regimen consisting of three drugs to achieve the complete eradication of H. pylori and a proper assessment of results.[24] Our study also has some limitations including a low number of patients and consequent risk of a statistical Type II error and follow-up of only up to 3 months. Based on the results of the present study, it can be summarised that the etiopathogensis of functional dyspepsia is heterogeneous in nature. H. pylori plays a significant role in causing symptoms of functional dyspepsia. Patients must be investigated for H. pylori and treated properly. Treatment of H. pylori infection with triple drug regimen in these patients brings a significant long-term improvement in the symptoms. In patients who are negative for H. pylori, other factors such as acid hypersecretion or psychological factors may play a role in causing the symptoms. Further studies are warranted in such patients to establish the exact cause of symptoms. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04087f3.jpg] [is04087t2.jpg] [is04087f1.jpg] [is04087t1.jpg] [is04087f2.jpg] [is04087t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}