 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
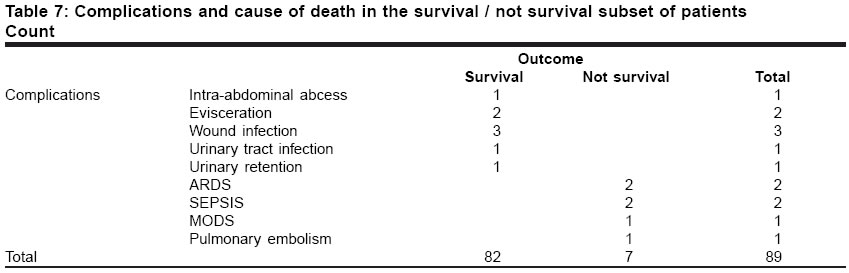
Indian Journal of Surgery, Vol. 66, No. 6, November-December, 2004, pp. 347-351 Original Article Penetrating abdominal trauma index: Sensitivity and specificity for morbidity and mortality by ROC analysis Gomez-Leon JoseFrancisco Department of Surgery, Division of General Surgery, Hospital Universitario Dr. Luis Razetti, Barcelona, Anzoategui Code Number: is04088 ABSTRACT BACKGROUND: When developed in 1981 by Moore and colleagues the Penetrating Abdominal Trauma Index (PATI) was used to identify trauma patients at risk of postoperative complications. Methods of trauma quantification have been extensively developed but their outcome evaluations have been naïve, subject only to basic statistical analyses. The accuracy of PATI was assessed by means of Receiver Operating Characteristics (ROC) curve analysis.AIMS: To evaluate PATI by means of ROC curve analysis and establish its sensitivity and specificity for predicting the morbidity and mortality in penetrating abdominal trauma. SETTINGS AND DESIGN: Patients who attended the University hospital trauma unit; prospective cohort study. METHODS: This was a prospective study over an 11-month period, patients with penetrating abdominal trauma who underwent laparotomy were enrolled. Initial assessment of the patients was done following the ATLS guidelines. Patients were stratified on the basis of those who developed complications, no complications and postoperative mortality. PATI was calculated based on operative findings and the outcomes were measured on the basis of complications or mortality in the postoperative period. STATISTICAL ANALYSIS: Receiver Operating Characteristics curve analysis and Logistic regression analysis using PATI as independent variable. RESULTS: Eighty-nine consecutive patients underwent laparotomy for abdominal trauma, 49 for stab wounds and 40 for gunshot wounds. Patients with complications scored a mean PATI of 21.47; those who died scored a mean PATI of 25.29. ROC curve analysis of PATI scores in patients who developed complications showed results of 42.1% sensitivity and 91.4% specificity. Sensitivity and specificity for mortality prediction was 42.9% and 91.5% respectively. CONCLUSION: The statistical evaluation of trauma scores should be performed using an adequate methodology to avoid naive evaluations. ROC curve evaluation of this trauma score index allows a comprehensive study of the instrument's performance, avoids data simplification and permits cross-analysis of different trauma score indexes. KEY WORDS: Penetrating Abdominal Trauma Index, ROC curve, instrument performance, Venezuela. The Penetrating Abdominal Trauma Index (PATI) is described as a method for quantifying the risk of complications following penetrating abdominal trauma, introduced in 1981 by Moore et al. PATI provided a useful means to investigate and served as a tool in the decision-making process when managing penetrating abdominal trauma.[1] In order to quantify trauma, injury severity instruments (ISI) are used in the different phases of trauma management for injury evaluation. Thus, pre-hospital triage instruments, in-hospital and outcome instruments are used to assess the level or type of care needed, for decision-making, and for evaluation of trauma outcome for policy decisions, respectively; that is why performance evaluation of these instruments have important clinical consequences.[2] ISI are evaluated via either naïve evaluations which depend upon the prevalence of the disease or outcome of interest in the study population, or calculations of sensitivity and specificity. Naïve assessments suppose the instrument′s performance in a single figure: accuracy prediction of events that are affected by prevalence-dependent populations that cannot be generalized, but can be valid within a specific study. Logistic regression analysis and sensitivity-specificity assessments avoid the aforementioned problems because they evaluate the instrument′s performance in two separate populations, where sensitivity equals the number of patients correctly predicted to live and specificity the number of patients correctly predicted to die, who actually die.[3] Several ISI have been correctly evaluated by means of these figures, these include the Injury Severity Score, New Injury Severity Score, ICD-9 codes and Revised Trauma Score. PATI lacks sensitivity, specificity or logistic regression analysis evaluations as evidenced in the available literature. It is being used as a powerful tool in our setting to asses penetrating abdominal trauma management. The goal of this paper is to evaluate this instrument′s behaviour, and study its ability to correctly prognosticate patients using the advantages of logistic regression analysis and ROC curve analysis over the traditional statistical techniques. MATERIALS AND METHODS The study was carried out in a university teaching hospital of Universidad de Oriente, Venezuela, in a prospective manner during a period of 11 months. Consecutive patients who arrived in the emergency room with penetrating abdominal trauma by stab wound or gunshot wound, and underwent exploratory laparotomy after evaluation by the general surgeon. Patients who had no lesion at laparotomy or died during the first 24 hours of the postoperative period were excluded. Each patient with penetrating abdominal trauma considered for laparotomy is assigned a PATI score after laparotomy abdominal evaluation in our centre. Patients received standard post-surgical care at the intensive care unit when needed and/or general surgical hospitalisation care if not amenable to the ICU. Complications and/or the cause of death were recorded and tabulated against the PATI scores. After laparotomy, PATI was assigned to each patient calculating the risk factor per organ injured and multiplying by the severity of injury estimate. Complications were recorded during the hospitalisation stay and this outcome was managed as a dichotomous variable, that is, patients who had postoperative complications and patients who did not have a complication until the time of discharge. The severity of trauma outcome was also analyzed as a dichotomous variable, thus, patients were stratified as survivors or deaths. Statistics: Mean score results for the two subsets of populations were obtained by analysis of variance (ANOVA) of the difference of points obtained by each subset of patients i.e. complicated vs. non-complicated and survival vs. non-survival. For logistic regression and ROC analysis PATI was used as the independent variable; complications and trauma severity outcome (death) were used as binary dependent variables, that is, binary response was set as complications present and no complications present until discharge and survival or no survival of patients. Logistic regression analysis was performed to determine the association of the relative predictive power of the independent variable with respect to the categorical dichotomous complication/no complication and survival/death dependent variables. ROC curve analysis was performed to summarize the instrument′s performance with respect to discriminating patients who will or not complicate and those who will or will not survive. Thus, mean PATI scores for each subset of the population were plotted and sensitivity/specificity calculated by means of non-parametric estimates of the Area under the curve. Statistical analysis was done using SPSS ® 9.0. Significance was attributed to P values < 0.05. RESULTS Eighty-nine consecutive patients admitted for penetrating abdominal trauma who underwent laparotomy were included in the analysis. The mean age was 27.10 ± 9.98 yrs. with a range of 14 to 69. Eighty-six patients were male, 3 patients female. 55.1% lesions were caused by gunshot wounds whereas 44.6% by stab wounds to the abdomen. PATI results in the Complications/No Complication subset of patients When stratified as subsets of populations, mean PATI score in patients who developed complications was 21.47 ± 12.97 (95% CI for mean PATI from 18.77 to 24.16), in contrast with those who did not complicate for whom the score was 11.24 ± 8.33 (95% CI for mean PATI from 9.50 to 12.97) [Table - 1]. [Figure - 1] depicts this, PATI separated complicated from non-complicated patients but overlapping is present. As obtained from the logistic regression model [Table - 2], we can assume that patients with PATI scores of 22 are 1.09 (95% CI 1.04 to 1.16) times more likely to present with complications than those with lesser score points, coefficient of PATI has a Wald statistic of 10.77 which is significant at the 0.001 level (99.9% confidence level). The overall model is significant according to the Model Chi-Square statistic (P = 0.0003). The model predicts 79.78 % of the responses correctly. The ROC curve analysis for this model gives an Area under the curve of 0.776 (95% CI 0.667 to 0.885) [Figure - 2], which makes this a fair test to discriminate complicated from non-complicated patients. At the score level of 22, the coordinates of the ROC curve [Table - 3] show a sensitivity of 42.1%, and specificity of 91.4%. PATI results in the Death/Survivors subset of patients Mean PATI score in patients who died was 25.29 ± 15.98 (CI 95% for mean PATI from 21.97 to 28.60), compared to the patients who survived (which account for all those who complicated and did not complicate) that was 12.41 ± 9.15 (95% CI for mean PATI from 10.50 to 14.31) [Table - 4]. [Figure - 3] shows how survivors are separated from non-survivors according to increasing PATI scores, although, overlapping exists as in almost all injury scores. The logistic regression model depicts that patients with this score of 25 or more are 1.08 (95% CI 1.02 to 1.16) times more likely to die when compared to patients scoring less points. Coefficient′s Wald statistic for PATI is 7.46, which is significant with a 99.4% confidence level (P = 0.006). Model Chi-square statistic assumes that the overall model is significant (P = 0.006) and the percentage of correct predictions rises to 93.26% [Table - 5]. Area Under the Curve for this model test is 0.787 (95% IC 0.626 to 0.948) [Figure - 4]; the ROC curve coordinates for cut-off values of 25 [Table - 6] give 42.9% and 91.5% sensitivity and specificity respectively, making this a fair model for prediction of mortality. [Table - 7] shows causes of complications and death in the patients who complicated and did not survive. DISCUSSION In our study, we could observe how increasing PATI score values correlate with complications in the postoperative period and even mortality secondary to complications; this is congruent with the published literature. Our aim was then to evaluate how this instrument′s performance fits with the standard statistical techniques currently used to asses the models. PATI has been used to measure injury severity in abdominal trauma in order to assist the surgeon in categorizing the patients at risk of developing complications, and even in decision-making techniques for repairing intra-abdominal organs according to its severity score.[4],[5],[6],[7],[8] Several methods to asses abdominal trauma have been evaluated with adequate statistical techniques that quantify sensitivity and specificity, but they include invasive approaches as laparoscopy or image studies.[9],[10] Among the trauma indices that have used this methodology of evaluation are the injury severity score and the new injury severity score.[2] A Trauma index instrument′s behaviour in categorizing a specific characteristic in trauma patients should be evaluated by a methodology that avoids data simplification and therefore bias in the conclusions obtained by its application. Logistic regression analyses allow evaluations on how an instrument′s performance can be graded with respect to the relative predictive power of a study variable on the effect of a specific characteristic outcome. ROC curve analysis evaluates an instrument′s performance in a comprehensive manner; as results are summarized in a simple way, this methodology avoids data loss and simplification.[2] This study supports the use of PATI as a useful method of quantifying penetrating abdominal trauma and as a predictor of complications and mortality, with an ample specificity level as confirmed by the ROC analysis. Limitations are those of the observational study type, as no experimental groups can be established, confidence evidence level is not the highest, but further robust statistical evaluations of the different trauma indices could produce enough evidence to set statements to encourage their use in the management of the trauma patients in our countries. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04088f4.jpg] [is04088t2.jpg] [is04088t5.jpg] [is04088t1.jpg] [is04088f3.jpg] [is04088t7.jpg] [is04088t4.jpg] [is04088t3.jpg] [is04088f1.jpg] [is04088t6.jpg] [is04088f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}