 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
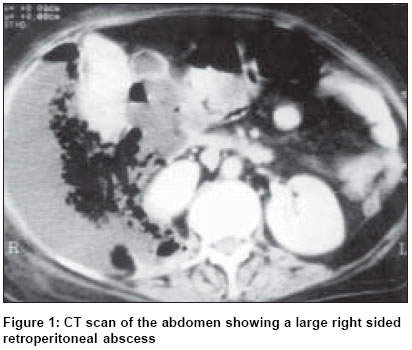
Indian Journal of Surgery, Vol. 66, No. 6, November-December, 2004, pp. 358-360 Case Report Choleretroperitoneum - An unusual complication of cholelithiasis Kaushik Robin, Attri AshokK Department of Surgery, Government Medical College and Hospital, Sector 32, Chandigarh - 160 030 Code Number: is04091 ABSTRACT Retroperitoneal abscess arising as a consequence of biliary tract disease has been termed choleretroperitoneum. It is rare, and was first reported about 170 years ago. Since then, only a handful of cases have been reported in English literature. The case of a 56-year-old female with a retroperitoneal abscess and colonic necrosis subsequent to gall bladder perforation is reported and the relevant literature is briefly reviewed. KEY WORDS: Gall bladder perforation, choleretroperitoneum, retroperitoneal abscess. INTRODUCTION Retroperitoneal abscesses commonly arise from the extension of a disease process of the retroperitoneal. Diseases of the duodenum, pancreas and the colon have been commonly implicated, but the biliary tract is one of the rare primary sites for the development of a retroperitoneal abscess. A retroperitoneal abscess arising due to biliary tract disease has been termed choleretroperitoneum. The exact aetiology of this condition is not known, but it is hypothesized that bile reaches the retroperitoneum either by rupture of the common bile duct (CBD), part of which is retroperitoneally situated, or by perforation of the gall bladder that is adherent to the posterior parietal wall. Posterior erosion of a pericholecystic abscess may also be a mechanism by which bile escapes into the retroperitoneum.[1] CASE REPORT A 56-year-old female, a known case of cholelithiasis, presented with a mass in the right lower abdomen, along with generalized abdominal pain and vomiting of 25 days duration. There was history of fluctuating fever during this period. She had had an attack of acute cholecystitis that required hospitalization, a week before the appearance of the abdominal mass. Examination revealed a markedly obese, dehydrated patient with tachycardia and tachypnoea. A large, tender and non-mobile mass was palpable in the right lumbar and iliac regions of the abdomen, extending from the right flank up to the umbilicus. There was no other significant finding on clinical examination. Investigations revealed haemoglobin of 9.7 gm/dl, with normal renal and liver functions, a prothrombin time index (PTI) of 75%, and a normal serum amylase. X-ray of the abdomen showed gas shadows in the right lower abdomen. Ultrasound of the abdomen showed a retroperitoneal fluid collection which on aspiration revealed thick pus. CT scan showed a large retroperitoneal collection with air pockets that were pushing the ascending colon and the right kidney medially and upward [Figure - 1]. The right kidney was also displaced medially. Surgery revealed a necrotic right colon that was pushed medially by a large retroperitoneal abscess. On mobilizing the ascending colon, one and a half litres of pus along with bile-stained necrotic material and a few large gallstones were drained. The gall bladder had thickened walls, and a large 1 cm x 1 cm perforation at the fundus that was densely adherent to the hepatic flexure of the colon and to the abscess cavity walls. Drainage of the abscess was followed by a thorough lavage, and a right hemicolectomy with ileostomy and mucous fistula. Partial cholecystectomy was also done. The patient developed wound infection and partial burst abdomen in the postoperative period, which were managed conservatively. There was also partial retraction of ileostomy that necessitated refixing of the stoma under local anaesthesia. Restoration of bowel continuity was done after six weeks, and she is presently well on a follow-up of nearly four years. DISCUSSION The retroperitoneum is a potential space between the peritoneum and the transversalis fascia along the posterior aspect of the abdominal cavity that is bounded by the diaphragm above and the pelvic brim below. The lateral margin of the quadratus lumborum muscle is its lateral extent, but medially it is in continuity with the retroperitoneal space of the opposite side. The retroperitoneal space is divided into the anterior retroperitoneum (containing the oesophagus, duodenum, pancreas, bile duct, portal and splenic veins, appendix, ascending and descending colon and the rectosigmoid) and the posterior retroperitoneum that contains the kidneys, ureters, aorta, inferior vena cava, lymph nodes and the gonadal vessels. Retroperitoneal abscesses commonly arise from an extension of the inflammatory processes of the organs situated within.[2] Diverticulitis, retroperitoneal appendicitis, pancreatitis, pancreatic cancer and peptic ulcer disease are the commonly implicated conditions in the development of retroperitoneal abscess, along with pyelonephritis and renal cortical abscesses. These usually present with an insidious onset and generalized symptoms, and the presence of physical signs indicates an advanced stage of abscess. A delay in diagnosis leads to a delay in instituting treatment, thereby contributing to increased mortality.[2] The biliary tract is a rare primary site for the development of retroperitoneal abscess. A thorough search of the available literature revealed a total of only 19 previously documented cases of choleretroperitoneum (perforation of the gall bladder or part of the biliary tree into the retroperitoneum) since its first description in 1836.[1],[2]-[8]. Twelve of these cases had associated biliary tract disease in the form of cholelithiasis,[1],[2],[3],[4],[8] choledocholithiasis,[1],[2] cystic duct calculus[1] and carcinoma of the CBD.[1] CBD necrosis occurred in the setting of gallstone pancreatitis in one case[4] whereas in another, rupture of the CBD was attributed to abdominal trauma.[6] Spontaneous retroperitoneal rupture of the cystic duct,[5] gall bladder[1],[2],[7] or CBD[1],[8] were the mechanisms implicated in the other cases. No obvious pathology could be identified either at surgery or during autopsy in three cases[1],[3] - maybe the perforation site sealed following the release of intra-luminal pressure after the escape of bile.[5] The mechanism by which bile reaches the retroperitoneum has also been a matter of conjecture, especially since the gall bladder and the extrahepatic biliary tract (except the lower two-thirds of the CBD) are intraperitoneal in their course. Perforation of the lower part of the CBD can obviously cause bile leak into the retroperitoneal space. Another possibility could be that the adhesion of the gall bladder neck to the posterior parietal peritoneum might occur as a result of chronic inflammation.[1] Subsequent perforation here would then be able to account for bile in the retroperitoneum rather than intra-peritoneally. Jacob et al felt that erosion of a pericholecystic abscess posteriorly was also a possible mechanism of bile leak into the retroperitoneum.[1] In the present case, we believe that a pericholecystic collection may have ruptured into the retroperitoneum, with colonic wall necrosis occurring secondary to thrombosis of the meso-colic vessels. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04091f1.jpg] |
| |||||||||

{kind=link}