 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
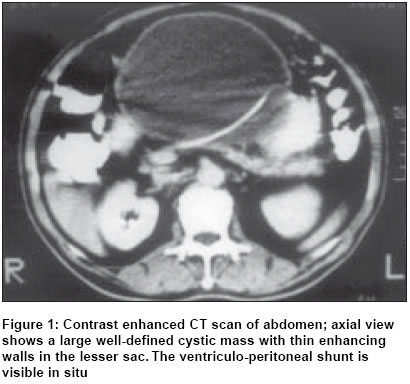
Indian Journal of Surgery, Vol. 66, No. 6, November-December, 2004, pp. 360-363 Case Report Abdominal CSF pseudocyst in a pateint with ventriculo-peritoneal shunt Sharma AlokK, Pandey AjayK, Diyora BatukD, Mamidanna Ravikrishna, Sayal ParagP, Ingale HarshalA Department of Neurosurgery, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai - 400 022 Code Number: is04092 ABSTRACT Abdominal cerebrospinal fluid (CSF) pseudocyst is an uncommon complication of ventriculo-peritoneal shunts. We report a case of a large lesser sac CSF pseudocyst in a 63-year-old male operated for fibroblastic meningioma of the cerebello-pontine angle ten years earlier. During the initial surgery a ventriculo-peritoneal catheter was inserted for associated hydrocephalus. He presented with epigastric pain and swelling since 4 weeks. A CT scan of the abdomen revealed a large cystic mass in the lesser sac with thin enhancing walls. An exploratory laparotomy was performed and the cyst drained externally with revision of the shunt. The patient had a rapid and uneventful recovery. We report this uncommon occurrence with a brief review of the literature. KEY WORDS: Cerebrospinal fluid, Pseudocyst, Ventriculo-peritoneal shunt, Laparoscopy, Infection INTRODUCTION Abdominal cerebrospinal fluid (CSF) pseudocyst is an uncommon albeit well described complication of ventriculo-peritoneal (VP) shunts. Although infection and subsequent high CSF protein content have been postulated as aetiological factors, they still do not account for a vast majority of the cases. The aetiology and management of the condition is still a topic of debate. With the advent of laparoscopic techniques, there have been rapid strides in minimal invasive management of this condition. We report this uncommon complication in a patient with no objective evidence of infection and briefly discuss the aetiology and various modes of management. CASE HISTORY A 63-year-old male presented to us with complaints of pain in the epigastric region and dyspepsia since four weeks. He had noticed a visible distension of the upper abdomen with appearance of a lump since 2 weeks. The lump had gradually increased in size ever since. He had been operated 10 years earlier for fibroblastic meningioma of the cerebello-pontine angle. At the time of the prior surgery a VP shunt was inserted for the management of the associated hydrocephalus. He had been asymptomatic since then. Presently he had no history of fever, vomiting, hemetemesis, malena or foul-smelling pale stools. There was no history suggestive of raised intracranial pressure. He had been an alcoholic but had undergone de-addiction and had completely abstained since 5 years. On examination the VP shunt was patent and functioning. Fundoscopy revealed no abnormality. On abdominal examination a lump was noted in the epigastrium extending into the right and left hypochondrium. The lump was well-defined, smooth, non-tender and moving with respiration. It was dull to percussion. Serum amylase was normal being 76 Caraway units. Ultrasonography (USG) abdomen and pelvis revealed a large well-defined cyst in the lesser sac about 16 x 9.8 x 13.6 cm in size. A thin strip of pancreas was seen which appeared normal. There was no free fluid in the abdomen. An immediate computed tomographic (CT) scan of the abdomen and brain was done. The CT brain revealed no anomaly with the shunt in the ventricles. There was no impression of ventricular dilatation. The abdominal CT scan showed a large, well-defined cystic mass measuring 18.3 x 10.7 x 13.2 cm with thin enhancing walls (3-4 mm thickness) in the lesser sac just anterior to the pancreas displacing the stomach to the left. It showed a curvilinear structure (the shunt tube) within. The ventricular peritoneal (VP) shunt was seen traversing the abdominal wall and entering the cyst [Figure - 1]. The pancreas was normal and the peripancreatic fat planes well maintained. A diagnosis of CSF pseudocyst was thus suspected on the basis of history and radiological findings. The patient was taken up for exploratory laparotomy for external drainage of the lesser sac collection. The VP shunt was separated from the cyst and a shunt revision was performed. The pancreas appeared normal on visual inspection. The cyst fluid was clear, straw-coloured. It was sent for analysis. The analysis showed a total cell count of 3, all being lymphocytes. Proteins were 80 mg% and sugar 74 mg%. Cyst fluid amylase levels were normal i.e. 40 caraway units. The diagnosis was thus confirmed. The patient had an uneventful recovery. Postoperative USG abdomen showed minimal collection in the lesser sac. The drain was removed on the 5th day post-operatively with minimal fluid draining and the patient was discharged on the 7th day post operatively. On follow-up examination after one month no abnormality was detected. DISCUSSION Hydrocephalus is the final common pathway of a myriad of disease processes. Though a specific diagnosis cannot be ascertained in all the cases, it is generally agreed upon that impairment of CSF resorption or obstruction to the flow of CSF causes hydrocephalus. The traditional treatment of hydrocephalus consists of the placement of a CSF shunt to divert the excess CSF from the ventricular system. VP shunts are most commonly utilized. Shunt complications are reported to occur at a rate of approximately 26%.[1] Diverse complications associated with the peritoneal end of a VP shunt have been described. These include CSF loculation and cyst formation, perforation of the viscera, migration of the shunt, bowel obstruction secondary to adhesions and metastatic spread via the shunt.[2] CSF loculation may present as recurrent ascites, peritoneal cyst, omental cyst subphrenic loculation or lesser sac loculation as in our case. Abdominal CSF pseudocysts are an uncommon complication and the incidence varies from less than 1% to 4.5% of VP shunts.[3],[4] The exact cause of abdominal CSF pseudocysts is still debated. Predisposing factors for pseudocyst formation are multiple shunt revisions, silicon allergy and prior shunt/CNS infection. In a series of 12 patients, Gaskill et al reported that inflammatory process is a frequent predisposing factor.[1] In their series 16% of the patients had acute infection while 41.6% had past history of CNS infection. In a review by Rainov N et al, microbiologically proven infection was present in 30% of their cases.[4] The most common intra-abdominal response to infection is the sheathing of the peritoneal catheter. The CSF draining into these sheaths produces large intra-abdominal fluid-filled cysts. CSF ascites, which is often a differential diagnosis in such cases is an entirely different entity and is an excessive accumulation of CSF in the peritoneal cavity resulting from an inability of the peritoneum to absorb the CSF even in the absence of liver pathology. Pseudocysts can be differentiated from ascites by their characteristic displacement of the bowel gas pattern on abdominal films and by the absence of shifting dullness.[5] However, our patient had no objective/subjective evidence of acute infection or past history of CNS infection. Thus infection, while an important factor, is not likely to account for all cases of pseudocyst. Sometimes a pseudocyst may mimic appendicitis. However, the diagnosis is clearly evident on radiology. The most common presentation of the paediatric patients is with symptoms of elevated intracranial pressure and abdominal pain, whereas the adults have predominantly local abdominal signs. Typical presentation includes abdominal pain and/or distension, with nausea or vomiting. Manifest shunt malfunction is not a prominent feature. A small amount or no peritoneal fluid is found in the patient with a normally functioning VP shunt. Ultrasonographic evidence of a larger, localized or loculated collection is abnormal and suggests CSF pseudocyst. CT scanning, which provides accurate localization, has now replaced other imaging modalities as the modality of choice. The treatment involves exploratory laparotomy followed by surgical removal of the catheter with or without excision of the pseudocyst wall and placement of a new catheter intraperitoneally in a different quadrant or an intra-atrial shunt. In their series, Gaskill et al found that the cyst reabsorbed spontaneously without excision or aspiration once the CSF was diverted. The peritoneal cavity could then be used for shunting once the cyst had reabsorbed. This sometimes required conversion to an atrial or pleural shunt before reutilization of the peritoneal cavity.[1] Infected cysts generally resolve with antibiotics and surgical management. As an alternative to transabdominal cyst puncture and conventional surgical cyst resection, Deindl et al reported a case where laparotomy was not necessary and mere aspiration of cyst contents via distal catheter followed by insertion of the distal catheter into the right atrium was sufficient.[6] In 1995, Kim et al first described the laparoscopic management of a CSF pseudocyst, which involved excision of a portion of the cyst and repositioning the catheter within the peritoneal cavity.[7] Laparoscopic management reduces the risk of a laparotomy and the formation of intraperitoneal adhesions. Furthermore, laparoscopy allows visual confirmation of the adequate flow of the CSF from the end of the catheter after it is repositioned. The entire abdominal cavity can be assessed for the presence of adhesions and adhesiolysis undertaken whenever necessary. This allows placement of the catheter in the quadrant of the abdomen with the maximum absorptive surface.[8] This minimally invasive technique in the setting of a non-infected pseudocyst has proven to be safe, with results comparable to the conventional open technique. However, the long-term success rate is still unknown. In spite of the numerous complications, VP shunt remains the method of choice for long-term relief of raised intracranial pressure. Improved shunt devices and careful surgical techniques may lead to a decrease but not elimination of the incidence of these complications. A high degree of suspicion and careful clinical and radiological examination could help diagnose and treat CSF pseudocysts, minimizing major complications. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04092f1.jpg] |
| |||||||||

{kind=link}