 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
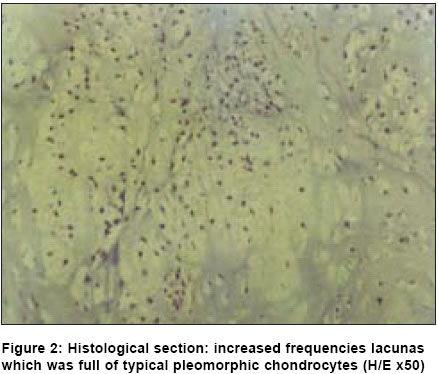
Indian Journal of Surgery, Vol. 66, No. 6, November-December, 2004, pp. 363-365 Case Report Chondrosarcoma in the forefoot Yildirim OmerSelim, Celik Hakan, Saruhan Onur, Gurhan Nesrin, Okur Ali Department of Orthopaedic Surgery, Ataturk University Medical Faculty, Aziziye Hospital, Erzurum Code Number: is04093 ABSTRACT Chondrosarcoma is a tumour rarely seen in the foot. An 18-year-old male patient visited our clinic with the complaints of swelling and pain in his right foot. On plain radiographs, there were lytic areas in the fifth metatarsal and the fourth and fifth fingers of the right foot. Computerized tomography revealed that there were mass lesions in the fourth and fifth fingers' phalanges, causing a wearing off irregularly limited to adjacent fat plans and hypodense calcifications the fifth metatarsus, occurring destruction in bone. An open biopsy was taken from the region of the lesion under local anaesthesia. Histopathological diagnosis was reported as low-grade chondrosarcoma. We applied ray amputation to the patient under general anaesthesia from the fourth finger disarticulation and the fifth metatarsus. In a 3-year follow-up, no local recurrence and metastasis were observed. The difference of our case from the ones reported in the literature is that the patient was young (18-year-old) and had a lesion involving two different compartments synchronously as localization.KEY WORDS: Chondrosarcoma, foot, phalanges, surgical treatment. CASE REPORT An 18-year-old male patient visited our clinic with the complaints of swelling and pain and shoe-pinch on the tips of his fourth and fifth fingers of the right foot, which had occurred nearly six months ago as a result of his trauma. Radiographs also detailed lytic areas in the diaphysis of the fifth metatarsal and the fourth and fifth fingers of the right foot, and there were mass lesions, having soft tissue overlap, causing expansion and destruction in the periosteum; there was pathologic fracture within the proximal phalangeal joint of the fourth finger [Figure - 1]. An open biopsy was taken from the fourth phalanges under local anaesthesia. In pathological examination, tumoral structure, consisting of pleomorphic cartilages cells eroding the bone as well as soft tissue elements in the sections, was observed. We applied ray amputation from the fifth metatarsus and the fourth finger disarticulation, under general anaesthesia, to the patient diagnosed as low-grade chondrosarcoma. In histopathological examination, hardening in lacunas with basophilic stroma in the sections, tumoral structure more than one atypical pleomorphic chondrocyte in lacunas, and slight myxoid changes in the matrix in the form of frayed foci were observed [Figure - 2]. It was diagnosed as low-grade chondrosarcoma. After the operation, the follow-up was done once in three months, with respect to local recurrence. In a 3-year follow-up, no local recurrence and metastasis were observed. DISCUSSION Chondrosarcomas of small bones like the hand and foot are rarely seen, and they may have potential of fatality.[1],[2] Damron et al (1995) reported only three cases (involving the feet and hands) among 2588 tumours.[3] Chondrosarcoma in the foot frequently involves the tarsal bones. The calcaneus and the fifth finger are the regions that are involved the most. The age distribution of the cases has been found to be mostly in the sixth and seventh decade.[5] Our case in the second decade shows a distinction in terms of sex distribution. Very few cases developing enchondroma secondarily have been reported in the literature.[6] It is very difficult to distinguish between enchondroma and chondrosarcoma because the pathologic appearance of both tumours in the hand and foot bones is similar. Pain is not used as a criterion in distinguishing chondrosarcoma from enchondroma. Radiological imagination is certainly valuable in diagnosis. Cortical destruction and soft tissue mass can be in permeative pattern.[6] The treatments of these two situations are certainly different from each other. Enchondroma is treated with either intralesional curettage or is left without treatment.[7] Metastasis and staging in chondrosarcoma are associated with histological grade and their prognosis depends on the histological grade of the tumour with sufficient treatment.[1] Effective treatment is crucial for avoiding recurrent incidence and depends on excising all tissues with carcinoma. As the tumour is radio-resistant, complete removal is the only treatment of choice. A wide excision for low-grade chondrosarcoma is generally advised. Following open biopsy, local excision or, if required, reconstruction is advised.[5] In our case, we think that the removal of the tumoral tissue from the normal tissue margin is the treatment of choice. Our case is a young case that had Grade 1 chondrosarcoma in his fourth and fifth finger and fifth metatarsal diaphysis. The difference of our case from the ones reported in literature is that he was young (18-year-old) and had a lesion involving two different compartments synchronously as localization. CONCLUSION Chondrosarcoma is a tumour rarely seen in the foot. Low-grade chondrosarcoma in an extremity can be treated with limited surgery. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04093f2.jpg] [is04093f1.jpg] |
| |||||||||

{kind=link}
{kind=link}