 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
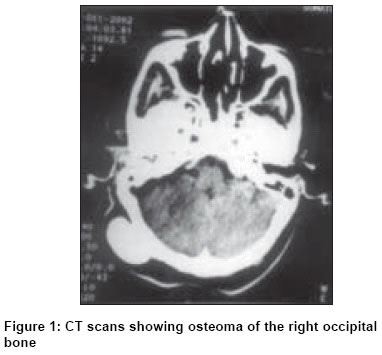
Indian Journal of Surgery, Vol. 66, No. 6, November-December, 2004, pp. 365-367 Case Report Osteoma of occipital bone Meher Ravi, Gupta B, Singh I, Raj A Dept. of ENT and Head and Neck Surgery, Maulana Azad Medical College and associated, L. N. Hospital, New Delhi - 110 002 Code Number: is04094 ABSTRACT Osteomas are benign, bone-forming tumours located within bones or developing on them. In the head and neck region they are commonly seen in the frontoethmoidal region. Occipital osteomas are very rare tumours. They are often asymptomatic and are incidentally found on radiological investigations. The main clinical symptom is headache of varying intensity and quality, though some patients may complain of dizziness in cases of large tumours. We describe here a case of occipital osteoma in a female, arising from the inner table. It was asymptomatic and osteoma was removed for cosmetic purpose. CT scan is a must to confirm the diagnosis, the involvement of the inner table as well as to look for any intracranial extent of the osteoma.KEY WORDS: Osteoma, occipital bone. CASE REPORT A 35-year-old female reported to the ENT OPD of Lok Nayak Hospital with a swelling on the right side of her head for more than 7 years. It was gradually increasing in size. There was no history of trauma, headache, hearing impairment, otorrhoea, dizziness, vomiting, visual trouble, or neurological deficit. On examination it was found to be around 4 cm x 3 cm in size, smooth, bony hard, and non-tender. X-ray skull showed a well-circumscribed dense bony mass. Her CT scan [Figure - 1] head revealed a bony mass in the right squamous part of the occipital bone measuring 4 cm x 3 cm. It originated from the outer table of the skull with no evidence of destruction of the inner table or extension of the mass intracranially. Hence, a diagnosis of osteoma was made. Surgical excision was carried out for cosmetic purposes using a chisel and mallet. It was arising from the outer table with a small stalk. The osteoma was attached to the underlying bone with a small stalk. The gross specimen [Figure - 2] was smooth, ivory white in appearance, ovoid in shape and about 4 cm x 3 cm in size. The histopathology report was osteoma composed of compact bone. The patient had an uneventful recovery with no recurrence in the 9-month follow-up. DISCUSSION Osteoma is a slow-growing tumour formed by mature bone tissue. Stuart first defined osteoma as a benign, circumscribed, slow-growing bony tumour[1] of mastoid. The common site for osteomas is the frontoethmoidal region. The incidence of osteomas is highest in frontal followed by, ethmoid and maxillary sinuses.[2] They are rare in the sphenoid sinus and extremely rare on occipital squama. A careful search of the English literature failed to reveal any previously reported case of occipital osteoma. Most often they are localized on sutures. Except for cortical lesions that are seen initially as cosmetic deformities, these tumours are usually unsuspected roentgenographic findings. The main clinical symptom is headache of varying intensity and quality, and in most cases not proportional to the size of the osteoma, which ranges from the size of a pepper bean to the size of a child′s head. In addition to headache, there can be sensitivity to pressure in the region of the frontal sinus or dizziness. Treatment is indicated for symptomatic osteomas. Tumours involving the middle and inner ear are most frequently small and tend to remain stable in size; consequently they are usually managed expectantly. Surgery is indicated in cases of deafness, discharge, dizziness and headache.[2] Temporal osteoma has been found to produce intracranial complications, justifying surgical removal. In our case the patient did not have any complaints, the swelling was removed for cosmetic reasons. The cause of osteoma has still not been defined. Since the tumour has been found to develop after puberty Haymann believed it to depend on conditions regulating growth in the cranial bones.[3] Friedberg suggested trauma with consequent periostitis as a predisposing factor.[4] Most authors feel that it originates from the pre-osseous connective tissue.[5],[6] The clinical presentation and radiological features of osteoma are characteristic but differential diagnosis should include eosinophilic granuloma, giant cell tumour, monostotic fibrous dysplasia, a solitary multiple osteoma, and osteoblastic metastasis.[7] One should also rule out Gardner′s syndrome in patients presenting with large skull osteomas.[8] It includes a clinical triad of familial polyposis coli, osteomas, and soft tissue tumours. CONCLUSION Osteomas are rarely rarely originate from the flat bones of the skull and their management depends upon the symptomology. Small osteomas are harmless and can be left as such; surgery is indicated only in cases of cosmetic problem. Large osteomas causing dizziness, headache and intracranial extension or compression, need excision. Differential diagnosis of other bony tumours should also be kept in mind while dealing with them. REFERENCES
Copyright 2004 - Indian Journal of Surgery The following images related to this document are available:Photo images[is04094f2.jpg] [is04094f1.jpg] |
| |||||||||

{kind=link}
{kind=link}