 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
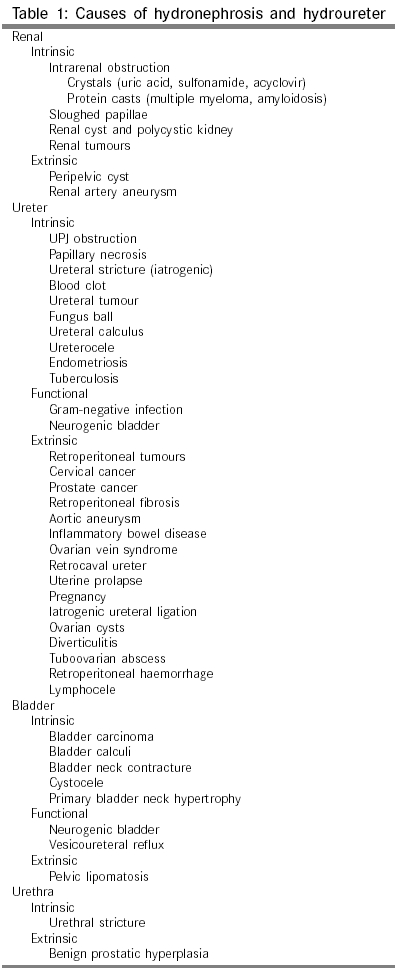
Indian Journal of Surgery, Vol. 67, No. 1, January-February, 2005, pp. 21-28 Review Article The obstructed kidney Nayyar Rishi, Sarda AnilK, Kaza RCM, Anand VJ Department of Surgery, Maulana Azad Medical College and Lok Nayak Hospital, New Delhi - 110 002 Code Number: is05003 Abstract Urinary obstruction is a common cause of acute and chronic renal failure. The symptoms and signs of an obstructed kidney may vary from asymptomatic to severe acute pain. The diagnosis and management of a hydronephrotic kidney is not very difficult with ultrasonography, IVU, and diuretic renography. The approach to manage such patients has been rationalized after the advent of diuretic renography. The obstructed kidney should be decompressed as early as possible because of progressive loss of renal function with prolonged obstruction. Nephrectomy may be required for a non-functioning kidney. Further advancements are being made as the molecular mechanisms involved in the pathophysiology of the obstructed kidney become known to us.Keywords: Obstructive uropathy, hydronephrosis, intravenous urography, diuretic renography, non-visualized kidney, non-functioning kidney, nephrectomy, ureteral stent, nephrostomy, postobstructive diuresis INTRODUCTION ′Obstructive uropathy′ refers to the structural impedance to the flow of urine anywhere along the urinary tract leading to ′hydronephrosis′, which is the dilation of the renal pelvis and calyces.[1] Dilatation of the renal pelvis can occur even in the absence of urinary obstruction; therefore, hydronephrosis and obstructive uropathy are not interchangeable or synonymous terms. The damage to renal parenchyma caused by these conditions often leads to ′obstructive nephropathy′ contributing to a decrease in renal function.[2] Unlike many other renal diseases, obstructive nephropathy, if treated early, is a potentially curable form of kidney disease.[3] INCIDENCE AND EPIDEMIOLOGY No data are available on the incidence and prevalence of urinary obstruction in unselected populations. In large surveys of elderly men a prevalence of 20-35% has been estimated for symptoms of urinary obstruction. Post-mortem examinations have found hydronephrosis in 3.8% of adults and 2.0% of children. Obstructive uropathy associated with congenital anomalies of the urinary tract accounts for 30-50% of all end stage renal disease cases in children.[4] In women, obstruction is more likely to occur at a younger age as a result of pregnancy or uterine cancer. Hydronephrosis is often discovered incidentally on an ultrasound conducted for another suspected abdominal disease. No definite data is available on this clinical entity and its clinical importance is uncertain, especially in Grade 1 or 2 hydronephrosis and in the absence of signs or symptoms of any disease. AETIOLOGY AND CLASSIFICATION There are a multitude of causes of hydronephrosis and hydroureter [Table - 1]. Urinary tract obstruction can be classified according to cause (congenital versus acquired), duration (acute versus chronic), degree (partial versus complete), and level (upper versus lower urinary tract). PATHOPHYSIOLOGY Obstructive uropathy occurs when the flow of urine is blocked at some point in the urinary tract, and urine accumulates above the obstruction. This increases the pressure and dilates the affected regions of the renal pelvis, calyces, and ureters. Increased ureteral pressure also results in pyelotubular, pyelovenous and pyelolymphatic backflow increasing the risk of systemic sepsis in the presence of infection. Hence, obstruction coexisting with infection should be considered a urological emergency. The dilated kidney is also more predisposed to trauma. The clinical profile of the patient varies according to the time interval over which the obstruction occurs (i.e. acute or chronic),
Acute urinary obstruction may produce little visible change in the collecting system or renal parenchyma. Chronic obstruction can produce an enlarged, normal or small atrophic kidney, again depending on the length and degree of obstruction, as well as the presence of an intrarenal or extrarenal collecting system. The intrarenal system, although obstructed to the same degree and duration as the extrarenal system, may not exhibit the same degree of hydronephrosis; however, the degree of renal damage may be worse. Usually, the collecting system dilates with time and the tissue between the calyces gets thinned out. Ultimately, the calyces coalesce with thin septa between them and a ′rim′ or ′shell′ of parenchyma remains peripherally. Microscopic changes consist of dilatation of the tubular lumen, flattening of the tubular epithelium and increased collagen deposition in the peritubular interstitium. Obstructive nephropathy can lead to kidney failure within a few weeks or a few years. Obstruction maintained for > 6 weeks results in hydronephrosis of the affected kidney with significant irreversible loss of functional renal parenchyma.[5] Renal function is also affected by relatively short-term obstructions.[6] Mustonen et al found that glomerular and tubular function partially improved during the first month following immediate correction of an obstruction.[6] However, months later, half the patients still showed glomerular damage, presenting as albuminuria, and tubular damage, presenting as elevated microglobulin alpha 1. Animal models have shown that the fibrotic and tubular apoptotic processes continue for a few weeks despite the reversal of obstruction.[7] CELLULAR INFILTRATES AND CYTOKINES IN URETERAL OBSTRUCTION Occupying nearly 80% of total renal volume, the tubulointerstitium, the area external to the glomeruli, tubules, and collecting ducts, appears to be the primary area where most damage caused by obstruction occurs.[8],[9] This is due to numerous vasoactive inflammatory mediators and growth factors which are released as the obstructive nephropathy causes mechanical damage to renal tissue. These include eicosanoids (e.g., prostaglandins, thromboxane A2), angiotensin II, atrial natriuretic peptide, nitric oxide (NO), endothelin, platelet activating factor, nuclear factor kappa B (NF~ kB), and transforming growth factor-beta (TGF-β).[8],[9],[10],[11] Cellular infiltrates typically involved in obstructive nephropathy include macrophages, T-lymphocytes, and fibroblasts.[8],[12],[13] With chronic obstruction, interstitial fibrosis develops, creating the most devastating and permanent effects on renal function.[14],[15] The prolonged imbalance between the mediators causes excess formation of protein in the interstitial matrix, while there is a deficiency in the mediators required for the destruction of protein. The net effect is overproduction of interstitial matrix, causing tubular atrophy and decreased numbers of functioning peritubular capillaries secondary to space displacement.[2],[15] Decline in both GFR and renal blood flow following obstruction is also caused by increased levels of thromboxane A2.[12],[16] Tubular cell damage occurs as a result of ischemia caused by reduced renal blood flow.[5] Damaged tubular cells further release substances which attract macrophages and also act on intact tubular cells to increase the production of additional inflammatory agents.[17] Although numerous biochemicals are involved in the process, one specific substance, TGF-β, is important.[8],[18],[19] It is released by macrophages and attracts fibroblasts, contributing to the development and proliferation of interstitial fibrosis.[9],[20] Recent evidence suggests TGF-β is the primary force driving the increased immunological response and the up-regulation of the renin-angiotensin system during the fibrotic process.[20],[21] TGF-β stimulates the production of NF~ kB, a factor associated with tissue inflammation, increased angiotensin II production, and the release of tubule cell chemoattractants.[22] It also promotes degradation of NO. Normally, NO protects the kidney from infiltration of macrophages into the interstitium and decreases the production of the protein interstitial matrix, suggesting it may have antifibrotic effects in the kidney.[4] Also, NO inhibits excessive vasoconstriction initiated by renin-angiotensin activation in processes like obstructive uropathy.[4] Angiotensin II exacerbates obstructive nephropathy by increasing TGF-β, which promotes both fibrosis and NO degradation.[17],[23] EFFECTS OF OBSTRUCTIVE UROPATHY ON GFR Three components determine the GFR: glomerular hydrostatic pressure, glomerular colloid osmotic pressure, and Bowman′s capsule pressure. All of these can be influenced by an obstruction. During the first few hours following obstruction, renal blood flow in the obstructed kidney increases secondary to preglomerular vasodilatation of renal blood vessels, which increases GFR.[1] As the GFR increases, increased urine formation begins to gradually increase ureteral pressure. About 4 hours into the obstruction, renal blood flow declines while ureteral pressure continues to increase associated with post-glomerular vasoconstriction.[1] Then, increased intrarenal pressure activates the renin-angiotensin system and increases levels of vasoconstrictors such as thromboxane A2, which results in decreased renal blood flow and a decrease in ureteral pressure associated with pre-glomerular vasoconstriction.[2],[8],[17] Bilateral ureteric obstruction (BUO) differs from unilateral ureteric obstruction (UUO). While during UUO, the kidney passes through these three phases, in BUO the kidney passes through a phase of pre-glomerular vasodilatation and then a post-glomerular vasoconstriction and remains in this state. Therefore, BUO is associated with progressive and persistent rise in ureteral pressure despite a decrease in renal blood flow. Postobstructive diuresis This phenomenon refers to the marked polyuria that occurs after the relief of BUO or obstruction of a solitary kidney. It is most often seen in patients who have chronic obstruction, volume overload and sometimes uremic encephalopathy. Most patients exhibit both solute diuresis (caused by retained urea, sodium and water) as well as a concentrating defect. The mechanisms responsible for this inability to concentrate urine include high atrial natriuretic peptide levels and impaired renal response to vasopressin. CLINICAL FEATURES The signs and symptoms of urinary obstruction depend on the parameters already discussed. The differentiation between acute or chronic obstruction is purely clinical. Chronic obstruction is usually asymptomatic. When the obstruction is bilateral, patients may present with uremia. Most acute obstructive uropathies, on the other hand, are associated with significant pain or the abrupt diminution of urine flow. The severity of the pain depends on the rate of distention more than the amount of dilation of the renal capsule.[24] Patients describe a colic pain in the flank that increases with consumption of large amounts of fluid or following diuretic administration. Anuria frequently occurs in acute obstruction and less frequently in chronic situations.[25] Sometimes, in unilateral obstruction or partial bilateral obstruction, the patient may notice significant increases in urinary output independent of fluid intake related to the damaged kidney′s inability to concentrate urine.[1] The clinician needs to obtain a detailed history about the type and duration of symptoms, hematuria, lower urinary tract symptoms, previous urinary tract infections (UTIs), history of stone disease, family history of prostate or pelvic cancer, and urinary output patterns. The presence of infection should always be considered as it may require emergent drainage. Examination may reveal volume overload.[24] There may be a palpable abdominal mass with or without costovertebral tenderness, related to hydronephrosis. Hydronephrosis that causes the kidney to expand enough to become palpable usually is related to a chronic condition.[25] The bladder may be palpable secondary to obstruction low in the urinary tract. Women presenting with suspected urinary obstruction should always receive a complete pelvic examination, and both genders receive a rectal examination.[1] In pregnant females, symptoms of frequency, dysuria, nausea, vomiting or back pain may be present even in a normal pregnancy. So, urological management is required only in pregnancy hydronephrosis complicated by strong flank pains or urolithiasis or pyelonephritis.[26],[27] LABORATORY EVALUATION Urinalysis results may be normal in both acute and chronic obstructions. Albuminuria may be absent but is commonly present in the range of less than 1.5 g/24 hours reflecting the increased glomerular permeability during urinary retention.[6] Even sparse albuminuria indicates glomerular dysfunction.[28] Microglobulin alpha-1, a low molecular weight protein, is an indicator of tubular dysfunction. Normally, nearly all microglobulin alpha-1 filtered by the glomerulus is reabsorbed by the proximal tubule.[6] With renal calculus or tumour involvement, microscopic hematuria is possible, but gross hematuria is unlikely.[29] Chronic obstruction leads to renal tubule damage, and the urinary chemistry findings are similar to those in intrinsic renal failure. These findings include urinary sodium greater than 20 mEq/L, fractional excretion of sodium (FE Na) greater than 1%, urine to plasma creatinine ratio of less than 20 and urine osmolality less than 350 mOsm/kg H2O.[1] With acute obstruction the urinary chemistry values are similar to those in prerenal azotemia. These findings include urinary sodium less than 20 mEq/L, FE Na less than 1%, urine to plasma creatinine ratio of greater than 30 and urine osmolality greater than 500 mOsm/kg H2O.[25] Microscopic evaluation of the urine may reveal erythrocytes, leukocytes, and bacteria. Blood tests include complete blood counts, hematocrit, haemoglobin, serum electrolytes (Na+, Cl-, K+, HCO3-, Ca++, HPO4-, Mg++), creatinine, blood urea nitrogen (BUN), uric acid, albumin and ABG.[1] The WBC count assesses for possible inflammation or infection secondary to obstruction or neoplasm as a cause of the obstruction. The hematocrit is important to assess for anaemia related to chronic renal insufficiency.[29] Patients with increasing serum creatinine without significant proteinuria, and trace to moderate numbers of red blood cells in the urine should immediately be suspected of having an obstruction.[24] RADIOLOGICAL EVALUATION Ultrasonography has become one of the most important tools for assessing urinary tract obstruction because it is rapid, low-cost, safe and sensitive. It is the diagnostic modality of choice in pregnancy.[27] The test is 98% sensitive for detecting hydronephrosis, but the specificity is 78%.[30] Though operator-dependent, ultrasound detects the type and level of the lesion, shows hydronephrosis, can indicate pyonephrosis (echoes within the collecting system) and tells the thickness of the renal parenchyma as an indicator of the duration and severity of obstruction. Since up to 22% cases of hydronephrosis are not obstructive, there is room for error.[30] Dilation without obstruction may be seen in vesicoureteral reflux, chronic massive diuresis, extrarenal pelvis, calyceal diverticula, congenital megacalyces and ileal conduits. Obstruction without dilation may be seen in intrarenal crystals, nephrocalcinosis, staghorn calculi and retroperitoneal obstruction. Use of duplex Doppler ultrasonography allows determination of the renal resistive index (RI), [peak systolic velocity - lowest diastolic velocity] / peak systolic velocity. An RI in the obstructed kidney that is 0.1 greater than the contralateral kidney is considered significant enough to indicate obstruction. The RI along with the colour Doppler to show the ureteral jet phenomenon, has improved the efficacy of ultrasonography in the diagnosis of renal obstruction in patients presenting with acute renal colic and for whom an IVU is not desirable e.g. pregnancy, history of contrast-induced allergy or renal failure.[31],[32] A supine radiograph [KUB] of the abdomen can reveal radio-opaque urinary tract calculi as the cause of obstructive uropathy.[33] However, alone it does not prove the calculi to be the cause of obstruction, it misses out radiolucent calculi and radio-opacity due to any other cause can be mistaken for the urinary calculi. Intravenous urogram (IVU) has been the gold standard for the detection of ureteral obstruction. The significant difference in IVU compared with ultrasonography is that the IVU shows both increased anatomic detail and functional attributes of the urinary system.[1] It tells about the exact site of obstruction, its cause, the degree of hydronephrosis, the status of renal parenchyma, guides the best treatment option, and also helps in deciding the best surgical approach for a particular patient. However, in view of nephrotoxicity of the contrast material, the usefulness of the test for patients already suspected of having obstructive nephropathy is questionable.[30] Also, poor renal function may render the test useless because of non-excretion of contrast. In general, a serum creatinine level of less than 2 mg% is needed. Another dilemma with IVU is the significant time requirement, up to several hours, for performing serial delayed films. Still, IVU remains the most widely used imaging modality to guide the management of patients of obstructed kidney, because of its low cost and easy availability. A kidney which is non-visualized on IVU (absence of both nephrogram and pyelogram even on delayed films taken after 24-72 hours) should be assessed with a renal scan before labelling it as a non-functioning kidney (single kidney GFR which is not sufficient to take care of body wastes). A kidney may be non-visualized on IVU because of renal agenesis, post-nephrectomy, poor function with or without obstruction, or even in the presence of normal function during renal colic leading to renal artery spasm. Non-contrast computerized tomography (CT) scan is an effective imaging tool for acute renal obstruction. With spiral scanners, images can be performed effectively without contrast media, take only 5 to 10 minutes to perform, and cost about the same as IVPs. In terms of benefits, the CT equals the accuracy of the IVP in determining the presence of obstruction, but surpasses the IVP in detecting the specific cause of the obstruction.[34] Various signs of obstruction on spiral CT include hydroureter, perinephric stranding, hydronephrosis, periureteral oedema and renal swelling. However, a non-contrast CT does not indicate function of the kidneys. MRI gives no added advantage over CT scan. In addition it does not visualise the stone. However, it correctly identifies the point of obstruction and the non-calculous causes of obstruction. MR excretory urography is a promising technique which affords equivalent functional and additional anatomical information to isotope renography. It is more accurate than Doppler ultrasound in the assessment of ureteric obstruction in pregnancy and is not associated with any risk of exposure to radiation, unlike IVU or renal scan.[31],[35] Renal scan and diuretic renography is the most reliable technique to quantitatively assess the split and total renal function in the presence of hydronephrosis. It is a non-invasive study, can be done even in patients with deranged renal function, has no risk of contrast-induced nephrotoxicity and also has much less radiation exposure than IVP or CT scan. It can also be used to measure differential function and, therefore, is useful for treatment planning. Moreover, a functional obstruction can be differentiated from an anatomic cause. It can be used to follow up a patient after relief of obstruction. Also, the assessment of renal blood flow provides a sense of whether function may return upon relief of the obstruction. However, images from these scans lack the resolution to define the site of obstruction. The current radiopharmaceutical agent most widely used is technetium-99m diethylenetriamine pentaacetic acid (99 mTc-DTPA). It is excreted by glomerular filtration and is not secreted or reabsorbed by the renal tubules. Another much more expensive agent is 99 mTc-mercaptoacetyl-triglyine (MAG3), which offers better anatomical resolution, is more efficiently excreted by the kidney (glomerular + tubular secretion), can be used in case of decreased renal function, and delivers a lower dose of radiation. Thus it is the agent of choice. This study involves injecting a radioisotope and monitoring its passage through the upper urinary tract. The early uptake of the kidney can be measured and indicates unilateral function. The clearance of the radiopharmaceutical agent from the renal pelvis with a T1/2 of <15 min is considered normal, between 15 to 20 min is equivocal and T1/2 >20 min indicates obstruction. Lasix (1 mg/kg) is then administered after approximately 20 minutes into the study if washout appears delayed. It is called as F+20 technique of diuretic renography. Progressive accumulation despite furosemide administration confirms obstruction. However, rapid emptying despite an initial delayed excretion indicates dilatation without obstruction (functional obstruction). A partial excretory response may indicate either partial obstruction or renal dysfunction with an inability to respond to diuretic. These can be differentiated by the F-15 technique of diuretic renography i.e. by administering the diuretic 15 min before the radiopharmaceutical agent. The equivocal response to diuretic due to poor response to diuretic in the F+20 technique, gets converted to washout response in this F-15 technique. A recent study has shown no differences in the renogram patterns of F+0 (giving diuretic and radiopharmaceutical together) and F-15 investigations.[36] Because the F+0 study is more practical and shorter, F+0 method is suggested when equivocal results are obtained by an F+20 study or as a single test when there is only one opportunity to confirm or exclude the presence of obstruction. The Whitaker test was considered gold standard for the evaluation of upper urinary tract dilatation, classically used for UPJ obstruction. But with the advent of diuretic renogram it is not often utilized clinically. It is an invasive test requiring a percutaneously placed cannula inside the renal pelvis and a bladder catheter connected to a pressure transducer each. Fluid (saline + contrast) is pushed into the renal cannula at the rate of 10 ml/min. Fluoroscopic monitoring of the anatomic site of obstruction can also be done. The rise of pressure in the renal pelvis to less than 15 cm H2O is non-obstructed, 15 to 22 cm H2O is equivocal and greater than 22 cm H2O is diagnostic of obstruction. Retrograde pyelogram does not interfere with renal function. However, this procedure requires anaesthesia and is associated with the risk of introducing infection in an obstructed system. It now has only an adjunctive role in the operating room during ureterorenoscopy or DJ stenting. Other investigative procedures may be required depending on the cause of obstruction, for example cystoscopy, evaluation for prostatic disease, and micturating cystourethrography for urethral stricture or a suspected vesico-urethral reflux. Urine culture and sensitivity should always be obtained in infected cases. MANAGEMENT Any urinary obstruction should be relieved if the patient is symptomatic, associated with infection, high-grade obstruction or a bilateral obstruction associated with elevated BUN and creatinine or uremia. Such patients should be treated on priority basis without undue delay because of progressively increasing renal loss with increasing duration of obstruction, as discussed above. The cases associated with infection should be dealt with urgently. Minimal intervention in the form of percutaneous nephrostomy or DJ stenting is the safest yet lifesaving procedure in such patients. Decompression of the urinary tract Decompression of the urinary tract is required when the definitive management of the disease which has caused the obstruction, is postponed for some period. It is also indicated in pregnancy, when the conservative treatment with analgesics and antibiotics fails, non-resolving infection, deteriorating renal function or absence of Doppler evidence of ureteral flow or an increased RI.[26] It may also be indicated when one is not sure of the functional status of the obstructed kidney. When urine collected from a decompressed system is greater than 400 ml and shows normal creatinine clearance, subsequent definitive surgery is indicated to correct the obstruction. Intrarenal obstruction secondary to crystals or protein casts is not amenable to surgical drainage. Maintenance of adequate hydration to promote high rates of urine output to dilute crystals and casts is the main treatment. Decompression of the upper urinary tracts (kidney, ureter) is accomplished by cystoscopic placement of a ureteral stent (distal ureteral obstruction) or percutaneous nephrostomy (proximal or midureteral obstruction). Decompression of the lower urinary tract is accomplished by urethral catheterisation or suprapubic catheterisation (open or percutaneous). Other measures to be performed when the patient is first seen include
DEFINITIVE MANAGEMENT The first crucial decision to be made is whether to remove the kidney or relieve the obstruction. Diuretic renography, ultrasonography (cortical thickness) and possibly even CT may help the clinician in deciding this, but the experience of the surgeon in assessing a clinical situation and per-op findings is the first. At times, laboratory data may seem to favour salvage, whereas the experience of the urologist favours nephrectomy. On the other hand, there have been cases of return of renal function when the kidney was salvaged if cortical thickness was adequate, even though pre-operative renography depicted poor renal function.[37] Nephrectomy should be considered if there is permanent severe loss of ipsilateral renal function (less than 10% of total renal function) or there is development of unmanageable complication in hydronephrotic kidney, e.g. severe recalcitrant infection (i.e.. pyonephrosis), or trauma to hydronephrotic kidney. The issue of renal salvage is more pressing if the patient has bilateral renal obstruction. Many a times a non-functioning kidney due to a benign cause is detected incidentally. Such a kidney warrants nephrectomy if it is associated with any of the following- intractable pain, stone disease, haematuria, recurrent infection, uncontrolled hypertension, malignancy, tuberculosis or large hydronephrotic kidney liable to trauma. The definitive management with the decision to preserve the kidney, depends upon the particular cause of obstruction and may include watchful waiting, endourologic approach, percutaneous minimally invasive technique, laparoscopic or conventional open surgery. Today the emphasis is on saving as much of the functioning renal tissue as is possible. When both kidneys require surgical correction, one cannot allow the time-honoured dictates to be followed. Although it is sound advice to operate on the symptomatic or the better functioning kidney first, the opposite kidney cannot be allowed to deteriorate further. It is imperative that the function of the other kidney be sustained by insertion of a DJ stent or a PCN catheter just prior to the time when a definite operative intervention is planned for the symptomatic/better functioning kidney. More experienced surgeons have also repaired both sides at the same sitting in the past. But its routine application is questionable. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05003t1.jpg] |
| |||||||||

{kind=link}