 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 67, No. 3, May-June, 2005, pp. 127-130 Original Article Five-year duplex follow up of femoropopliteal percutaneous transluminal angioplasty Dalmia S, Pathak R1, Callum K2 George Eliot Hospital, Nuneaton, UK, 1Royal Free Hospital
and Medical School, London, UK and 2Derbyshire Royal Infirmary, Derby,
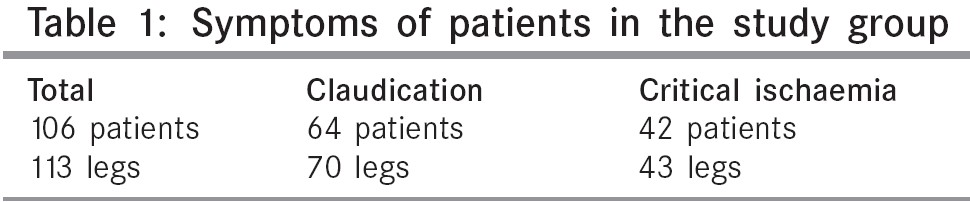
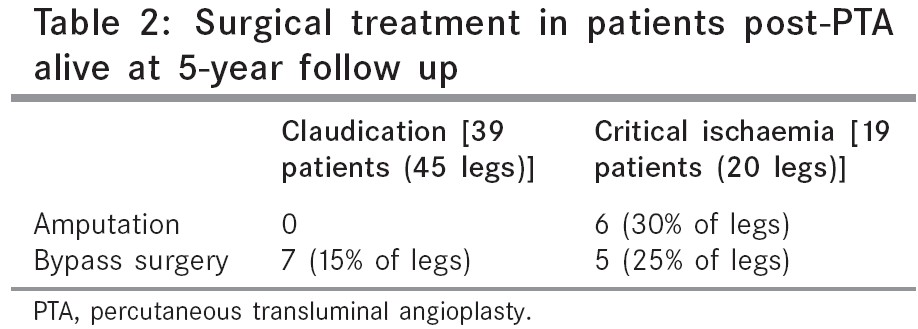
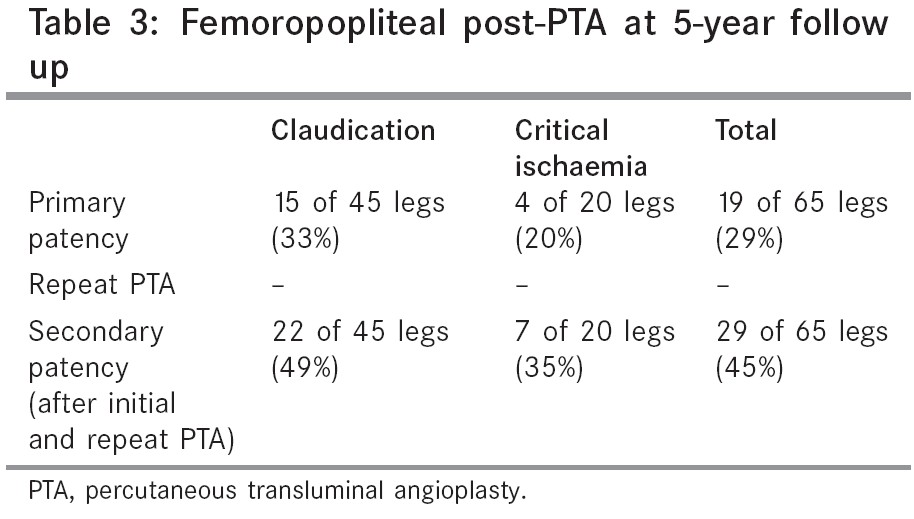
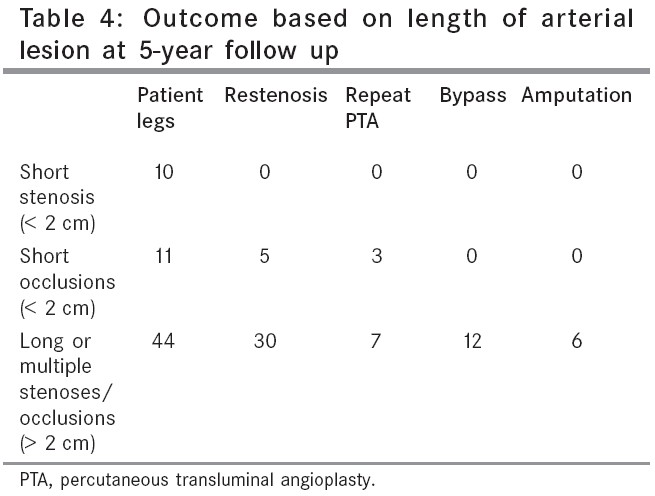
UK. Code Number: is05035 Abstract OBJECTIVE : To assess the 5-year patency of femoropopliteal percutaneous transluminal angioplasty (PTA) performed in a District General Hospital. Keywords: Chronic peripheral arterial occlusion, percutaneous transluminal angioplasty, duplex ultrasound, bypass surgery, amputation Since its introduction in 1964[1] and modification 10 years later,[2] percutaneous transluminal angioplasty (PTA) has been widely used. Its efficacy is accepted in iliac disease.[3],[4] Its use in the femoropopliteal segment is far more controversial. Some reports have shown good results with this procedure.[5],[6] Comparison of PTA and surgical revascularization for femoropopliteal disease shows a better patency than bypass using PTFE.[8] Some studies have suggested that angioplasty may have short-term benefits but that they are not sustained.[9],[10] The object of this study therefore was to study patients 5 years after femoropopliteal PTA using duplex ultrasound to obtain accurate results regarding vessel patency. Patients and methods All patients who had femoropopliteal PTA performed in the years 1993-1995 were identified from the hospital records. This study group consisted of 106 patients (65 males, 41 females) with a mean age of 70.5 years (range 28-90). The notes were examined to identify those who had died, had bypass surgery or an amputation. The surviving patients were contacted and invited to a special clinic in the vascular laboratory where they were questioned clinically by authors and where a duplex ultrasound was performed by one of three vascular laboratory technicians.Results One hundred and thirteen lower limbs PTA's were performed in 106 patients in the period 1993-1995. Technical failure occurred in 11 patients giving a technical success rate of 102 of 113 (90%). Major complications occurred in four patients (3.5%). The complications which occurred were embolic occlusion in two and local thrombosis at the site of angioplasty in two. Of the initial 106 patients, 64 had the procedure performed for claudication and 42 for critical ischaemia [Table - 1]. Thirty-six of the 106 patients had died at 5 years (34%), 19 of these were claudicants (18%), and 17 were patients with critical ischaemia (16%). Twelve patients were lost to follow up; six in the group with claudication, leaving 45 legs for study and six patients with critical ischaemia were also lost to follow up leaving 20 legs for study. Lower limb bypass was performed in 12 patients of whom seven were patients with claudication (15%) and five patients with critical ischaemia (25%). No patient who had angioplasty performed for claudication ended up needing an amputation, but six patients with critical ischaemia did need a major amputation (30%) [Table - 2]. A repeat PTA was performed in ten patients, seven who had claudication (15%), and three with critical ischaemia (15%). This gave an overall primary patency rate of 19 of 65 legs (29%). Out of those for whom the procedure was performed for claudication, primary patency was 15 of 45 (33%), and of those with critical ischaemia was 4 of 20 (20%). However, the overall secondary patency in patients who had had a repeat PTA was 29 of 65 (45%) and was 22 of 45 (49%) for claudicants, and 7 of 20 (35%) with critical ischaemia [Table - 3]. A further study of the arteriogram was performed to see whether there was any difference in outcome in patients with a stenosis or an occlusion and whether the length of the lesions made any difference. Patients with lesions of 2 cm or less were compared with those who had longer lesions [Table - 4]. There were ten limbs, which had a stenosis of 2 cm or less and of these only two developed a restenosis and none needed repeat PTA or any subsequent surgery. There were 11 with occlusion of 2 cm or less of which five developed a restenosis and of those three had a repeat PTA but none required bypass surgery or amputation. However, of the 44 limbs, which had long or multiple lesions, both stenosis or occlusions, 30 developed restenosis of which seven had a repeat PTA, 12 required a bypass operation, and six required major amputations. Discussion This study confirms the generally poor long-term results of femoropopliteal PTA with a primary patency rate of 29%. However, the secondary patency of 45% is more encouraging. All of the ten PTAs performed for single short stenoses were still patent 5 years later and only two had developed further stenoses, neither of which was severe enough to have further treatment. Of the 11 that had a single short occlusion, five developed a restenosis, but three of these were able to have a successful repeat PTA and none required bypass operation or amputation. This is comparable to 5-year results for lower limb bypass surgery.[11] Thus, one can conclude that for short lesions the results are sufficiently good to perform femoropopliteal PTA. It should be borne in mind that many patients with claudication develop a spontaneous improvement due to the development of collaterals,[12] although the process may take up to 6 months or more. During this time, it is certainly important to persuade them to give up smoking and to control their blood pressure. There is also evidence that lowering lipids may improve both their symptoms and the deterioration of the underlying disease.[13] They should also be encouraged to exercise as much as they can, as there is evidence that this helps. If, after this conservative treatment, patients' symptoms have not improved sufficiently, then duplex ultrasound can be used to demonstrate those patients with short-arterial lesions in whom a good long-term result from PTA could be anticipated. Of those with critical ischaemia, it will be even less common that they will have a short lesion that is amenable to angioplasty. However, the majority of patients with critical ischaemia have disease at several levels and even if the more significant lesion may be in the tibial vessels, good improvement can still be obtained in many patients by performing an angioplasty of a more proximal lesion in the iliac, Femoral or popliteal segment.[14],[15] In these patients, our studies would suggest that one could be fairly hopeful of an acceptable long-term result. The poor results for PTA of the longer or multiple lesions preclude its use for intermittent claudication where the patient should be treated conservatively with exercise programmes,[9] lipid lowering,[13] and antiplatelet treatment.[16] Should these measures fail to improve them sufficiently, then they can be considered for bypass surgery. With regard to critical ischaemia with longer or multiple lesions, once again the long-term results are unlikely to be good. Those patients who are fit enough and in whom the lesions are suitable for bypass surgery should have this performed. However, there are some patients who are heading for an amputation and yet are very unfit for any form of surgery in whom it is still unjustifiable to perform a balloon angioplasty for these longer or multiple lesions. Our results show that a repeat PTA or a bypass may still be possible later and one must remember that such patients usually have a very limited life expectancy. Therefore, it is reasonable to perform a procedure, which may only have short-term benefits, particularly in view of the associated low mortality and morbidity of PTA. This has been confirmed in a recent study from Sweden.[17] There are randomized controlled trials that have shown that Duplex ultrasound as early as 1 day postangioplasty can predict failure at 1 year.[18] One randomized trial from USA has shown that improved patency after PTA did not necessarily translate into clinical improvement compared to exercise alone.[19] It is important to note that all angioplasties in our study were performed using a transluminal technique. There is some evidence that the results of angioplasty for long lesions may be improved using a subintimal technique.[20],[21] References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05035t4.jpg] [is05035t3.jpg] [is05035t2.jpg] [is05035t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}