 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 67, No. 3, May-June, 2005, pp. 131-134 Original Article Laparoscopic cholecystectomy during pregnancy Singh Kuldip, Ohri A, Juneja S Department of Surgery, Dayanand Medical College & Hospital,
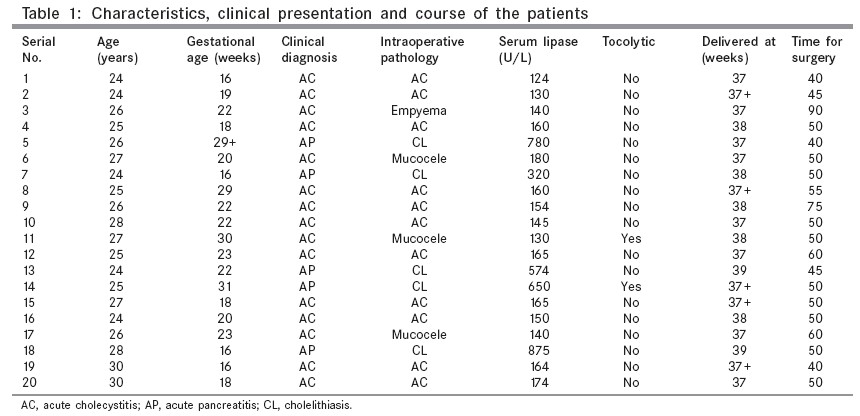
Ludhiana, Punjab, India Code Number: is05036 Abstract INTRODUCTION: Acute cholecystitis is the second most common nonobstetric emergency during pregnancy, after acute appendicitis. Once considered to be a contraindication to laparoscopic cholecystectomy in the past, several recent reports have documented the successful use of laparoscopic cholecystectomy during pregnancy. This study shows our experience of laparoscopic cholecystectomy during pregnancy in 20 patients. Keywords: Laparoscopic cholecystectomy, pregnancy Acute cholecystitis is the second most common nonobstetric emergency during pregnancy, after acute appendicitis. Gallstones are present in approximately 5% of the pregnant population and often are symptomatic.[1],[2] Multiparity increases the risk of the formation of gallstones.[3] Most patients with cholecystitis can be managed conservatively until the postpartum period; however, conservative management is associated with high recurrence rate and approximately half of the patients require rehospitalization.[1],[4],[5],[6] Some authors have reported a higher incidence of spontaneous abortion, preterm labor, or premature delivery in patients treated with nonoperative therapy than those undergoing cholecystectomy.[1],[4],[7] Cholecystectomy is required in approximately 0.05% of all pregnancies and in 40% of pregnant patients with gallstone disease.[2],[5],[8] Although pregnancy was once considered to be in the past, a contraindication to laparoscopic cholecystectomy, several recent reports have documented the successful use of laparoscopic cholecystectomy during pregnancy.[9],[10] This study shows our experience of laparoscopic cholecystectomy during pregnancy in 20 patients. Material and methods During the period of January 1993-2004, we have operated upon 20 pregnant patients with symptomatic gallstones, 16 of whom were operated in the second trimester and four were operated in the third trimester. Indications of cholecystectomy in pregnant patients included recurrent attacks of acute cholecystitis (patients who were managed conservatively on the first attack but who had a second episode of acute cholecystitis during pregnancy) and gallstone pancreatitis. The diagnosis was confirmed by ultrasonography and by pancreatic enzyme levels. All the patients were given general anesthesia. Care was taken to place the patient in 30° left lateral position with minimal reverse Trendelenberg to displace the gravid uterus away from the inferior vena cava thereby maintaining the venous return. After cleaning and draping the patient, abdomen was palpated under anesthesia to palpate the level of the uterus and the first port was placed in the supraumbilical position by open technique to create the pneumoperitoneum. Use of a Verres needle was avoided to prevent injury to the gravid uterus. In the second trimester, supraumbilical port placement did not pose any problem; however, we had to shift the umbilical port further up in the midline after palpating the uterus in case of patients in the third trimester. Rest of the ports were placed under direct vision as in the case of nonpregnant patients. Intra-abdominal pressure was kept as low as possible in the range of 10-12 mmHg, while maintaining the adequate visualization. We kept a drain for 24 h postoperatively in all the patients. Perioperative fetal monitoring was done and tocolytic agents were used only on the evidence of uterine irritability or contractions. Care was taken to avoid sedatives in the perioperative period. Only NSAIDs were used for postoperative analgesia and the use of opioid analgesics were avoided.Results Out of 20 pregnant patients who underwent laparoscopic cholecystectomy, 16 patients were in the second trimester and four were in the third trimester with a mean age of 28.5 years. Fifteen patients were operated for recurrent attack of acute cholecystitis and five patients underwent laparoscopic cholecystectomy for gallstone pancreatitis. In the third-trimester patients, two ( n = 2) patients were in the 29th week, one ( n = 1) was in the 30th week and one ( n = 1) was in the 31st week of gestation. The most common presentation was pain in the right upper abdominal quadrant with/without vomiting ( n = 15), and pain epigastrium with/without vomiting was the presenting complaint in five patients ( n = 5) [Table - 1]. Patients having acute pancreatitis were managed conservatively till clinical and biochemical recovery and laparoscopic cholecystectomy was done in the index admission in these patients with varying time interval from onset of pancreatitis, till the surgery (5-14 days). Mean operative time was 55 min, which varied from 40 to 90 min with a median of 50 min. Intraoperatively one patient had empyema of gallbladder ( n = 1), three patients had mucocele of the gallbladder ( n = 3), and 11 patients had acute cholecystitis, whereas five patients who presented with acute pancreatitis had only cholelithiasis with normal gallbladder intraoperatively. In all the patients, intra-abdominal pressure was kept less than 12 mm of Hg. All the patients went on to deliver at the full term; however, tocolytic agents were used in two patients in the 30th and 31st week but the contractions were controlled and they also delivered at the full term. There was no abortion or fetal loss, and no maternal mortality. There was no incident of fetal distress. All patients with no complications were discharged on the third postoperative day. The two patients having uterine contractions were discharged on the seventh and nineth postoperative day after ensuring the well being of the fetus.Discussion Once thought to be an absolute contraindication during pregnancy, laparoscopic cholecystectomy is becoming more widely accepted during pregnancy as evidenced by numerous favorable reports in the literature.[3],[11] Pregnancy is thought to predispose to gall bladder disease for a number of reasons. Estrogen plays a role in the predisposition as evidenced by the increased incidence of cholesterol stones in females. Women who receive exogenous estrogen, either as oral contraceptive or as postmenopausal estrogen replacement, are at a greater risk of developing gallstones due to increased saturation of cholesterol in bile. Progesterone causes the impaired response of the gall bladder to cholecystokinin. Therefore, pregnancy, by increasing the levels of female hormones predispose to gall bladder disease.[12] There are several issues, which have to be addressed before implementing laparoscopic cholecystectomy to the pregnant patients. Increased intra-abdominal pressure due to pneumoperitoneum and pressure from the gravid uterus on IVC may reduce the venous return, which can lead to decreased cardiac output and to reduced uterine flow. A combination of reduced uterine flow and increased intrauterine pressure secondary to pneumoperitoneum may lead to fetal hypoxia.[13],[14] Care was taken in our series to maintain 30° left lateral tilt with minimal reverse Trendelenberg position to maintain the adequate venous return. There has been an apprehension about carbon dioxide pneumoperitoneum potentiating the respiratory acidosis in the mother and the fetus.[13],[14] End tidal carbon dioxide monitoring has to be continued in the perioperative period to prevent acidosis. Use of alternate gas, such as nitrous oxide, to insufflate the peritoneal cavity has been proposed.[15] However, animal studies have shown that short-term fetal acidosis, even if severe, may not lead to deleterious effects.[16]
Intra-abdominal pressure has to be kept to a minimum while maintaining adequate visualization.[14] We could complete our cases successfully while maintaining the pressure in the range of 10-12 mmHg. Some authors have reported the use of gasless laparoscopy in patients who cannot tolerate the pneumoperitoneum and that the results were good, but the technique has a higher conversion rate than conventional laparoscopy.[17] Many authors have advised to place the first trocar just below the xiphisternum and then place the supraumbilical trocar under direct vision[18], or to use an optical trocar which allows the surgeon to see the tissue planes and the intra-abdominal organs as the trocar is advanced.[19] We complied with the open technique for the port placement to create the pneumoperitoneum with no bowel injury or uterine injury.[20] This technique has been advocated by many authors in the literature as the safest technique during pregnancy.[18],[20] However, in our series no case was presented in the first trimester, and the rate of abortion and preterm labor was zero percent in both second and third trimester, respectively which is in accordance to the reported literature.[18],[21] Opioid analgesics should be avoided during pregnancy for the fear of depressant effects on the fetus. The NSAIDs provide good postoperative analgesia. All the advantages of laparoscopic cholecystectomy exist for the pregnant patient also. Major advantages of laparoscopic cholecystectomy are earlier return of the gastrointestinal function, earlier ambulation, decreased hospital stay, and quicker return to routine activity. One potential advantage of the laparoscopic cholecystectomy over open cholecystectomy during pregnancy is that laparoscopy results in less manipulation of the uterus with adequate exposure, which lead to decreased uterine irritability and decreased preterm labor or delivery or spontaneous abortion.[2],[6],[19],[23] Conclusions Pregnancy should no longer be considered as a contraindication to laparoscopic cholecystectomy. All pregnant patients requiring cholecystectomy in second and third trimesters should be offered the advantages of the laparoscopic cholecystectomy, provided the specific issues of anesthesia, position of the patient, and surgical technique are addressed properly and meticulous perioperative monitoring is done.References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05036t1.jpg] |
| |||||||||

{kind=link}