 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 67, No. 3, May-June, 2005, pp. 135-139 Original Article Simplified criteria for predicting the severity of gallstone pancreatitis Singh Kuldip, Nain PS, Matta H, Ohri A, Chaudhry A, Jain M Department of Surgery, Dayanand Medical College and
Hospital, Ludhiana, Punjab, India Code Number: is05037 Abstract BACKGROUND: There was a need for a simple method of predicting the severity of gallstone pancreatitis soon after admission, to guide the clinician for intensive monitoring, or for transfer to a specialist center.AIM: To validate the role of simplified criteria [white blood cell count (WBC) > 14.5 x 103/dl; blood urea nitrogen (BUN) > 12 mg/dl; random blood sugar (RBS) > 150 mg/dl; pulse > 100/min] in predicting the severity of gallstone pancreatitis at admission. SETTING AND DESIGN: This prospective study was performed on 54 patients with gallstone pancreatitis admitted in the Department of Surgery of a tertiary hospital. MATERIAL AND METHODS: Fifty-four patients with gallstone pancreatitis were followed for development of complications. Sensitivity analysis of Biliary Ranson > 3, modified Imrie > 3, acute physiology and chronic health evaluation II (APACHE-II) score of > 5, WBC > 14.5 x 103/dl, BUN > 12 mg/dl, RBS > 150 mg/dl, pulse > 100/min and combinations of the four simplified criteria were compared using the Z -test. P < 0.05 was considered statistically significant. RESULTS: Both Biliary Ranson > 3 and modified Imrie > 3 had sensitivity of 96.15% and specificity of 96.43%. Both APACHE-II > 5 and RBS > 150 mg/dl had sensitivity of 88.46%, which is comparable to Biliary Ranson > 3 and modified Imrie > 3. CONCLUSION: RBS > 150 mg/dl can be used as a simplified prognostic indicator at admission in patients with gall stone pancreatitis and is comparable to Biliary Ranson > 3, modified Imrie > 3, and APACHE-II of > 5. Keywords: Gallstone pancreatitis, prognosis, random blood sugar The incidence of acute pancreatitis is increasing through the decades, and gallstones are responsible for most attacks. Although most patients recover uneventfully, a subgroup goes on to develop severe complications. The difficulty in predicting the likely course of the illness has been well described, and this unpredictability has led to the search for more objective methods of grading the severity. Numerous scoring systems namely: Ranson criteria,[1] modified Imrie,[2] and acute physiology and chronic health evaluation II[3] (APACHE-II) are the currently used prognostic indicators. But 48 h are required to complete the data collection for Imrie and Ranson criteria. Acute physiology and chronic health evaluation II scoring system is more complicated than either Ranson or Imrie and is therefore disadvantageous for routine application. There have been studies to find single-value predictive indicators in acute pancreatitis such as C-reactive protein, polymorphonuclear elastase, trypsinogen activation peptide, interleukin-6, carboxypeptidase-B, etc. All these studies required good diagnostic abilities in the institutes and were costly investigations, thereby limiting their use to advanced tertiary level institutes, and so there was a need for simpler and readily available prognostic indicators. Meek et al.,[4] in their study, have also tried to establish simplified criteria in predicting the severity of gallstone pancreatitis. In this present study, we tried to validate the four simplified admission criteria [white blood cell count (WBC) > 14.5 x 103/dl; blood urea nitrogen level (BUN) > 12 mg/dl; Pulse > 100 beats/min; random blood sugar (RBS) > 150 mg/dl] readily available at the time of admission in comparison to APACHE-II > 5, modified Imrie 3, or Biliary Ranson[5] > 3 in predicting the severity of gallstone pancreatitis. Material and methods In this prospective study, all the patients of gallstone pancreatitis admitted in the Department of Surgery of our hospital (54 patients) between January 2003 and October 2004 (22-month period) were studied. Patients were enrolled in the study after obtaining informed patient consent, and the study was approved by the Ethical Committee of the Hospital. The diagnosis of acute gallstone pancreatitis was based on the following
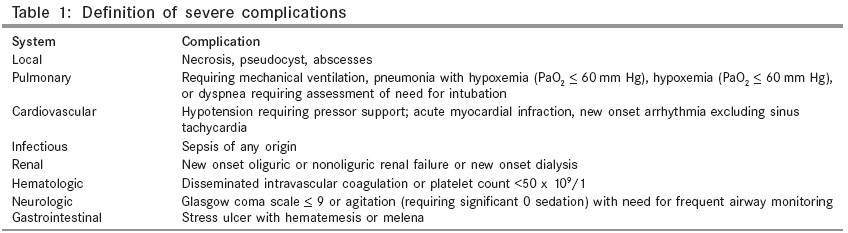
criteria: In all the cases, a detailed history was recorded. Patients with a previous history of diabetes mellitus were also excluded. This was followed by a detailed general physical and systemic examination. Physiological factors and laboratory data were collected on admission and recorded daily. All the patients were managed according to the current clinical guidelines and were monitored daily for evidence of severe systemic and local complications. Patients developing any of the complications listed in [Table - 1] were considered as patients with severe pancreatitis. The four criteria (WBC, BUN, Pulse, and RBS) were used as prognostic indicators at admission. The cut-off values for the above were:
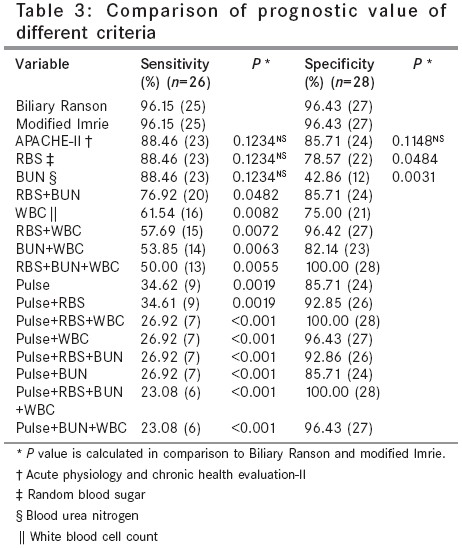
The APACHE-II,[3] modified Imrie,[2] and Biliary Ranson score[5] were calculated using the biochemical and physiological data. The sensitivity and specificity of each of the individual simplified criteria, combinations of simplified criteria, APACHE-II > 5, M. Imrie > 3, and Biliary Ransons > 3 were calculated. Comparison of sensitivity of different variables was done in comparison to Biliary Ransons and modified Imrie by applying the Z -test. Comparison of specificity of variables with comparable sensitivity was also done by using the Z -test. Z -test is a standard statistical test of proportions and is used to compare any two proportions. P < 0.05 was considered statistically significant. Results Out of the total 54 patients, 29 (53.7%) were females and 25 (46.3%) were males. The average age of the patients was 50 ranging from 14 to 85 years. Twenty-six patients (48.14%) developed complications [Table - 2] and were labeled as cases of acute severe pancreatitis, the other 28 patients (51.86%) being cases of mild pancreatitis. Fourteen patients (25.92%) developed local complications only, out of which 13 patients developed pseudocyst alone, and one developed necrosis. There was no mortality within these patients. Systemic complications were present in 12 patients (22.22%). Hypoxemia was the most common complication and it was present in 16.67%. Total number of mortality in this study was five (9.25%) and all these patients were associated with multiple organ system failure. Both Biliary Ranson > 3 and modified Imrie > 3 had a sensitivity of 96.15% (25 patients) and each of them missed one patient who developed local complications only. Both had a specificity of 96.43% (27 patients) and wrongly predicted only one patient as a case of severe attack. They were the most sensitive and specific indicator of severity in this study. Acute physiology and chronic health evaluation II > 5 had a sensitivity of 88.46% (23 patients, P = 0.1234NS) and it missed three patients who developed local complications. It had a specificity of 85.71% (24 patients, P = 0.1148NS) and wrongly predicted four patients to be cases of severe attack. RBS > 150 mg/dl had a sensitivity of 88.46% (23 patients, P = 0.1234NS) and it missed three patients out of whom two patients developed local complications and one developed systemic complication. It had a specificity of 75.57% (22 patients, P = 0.0484) and wrongly predicted six patients to be cases of severe attack. BUN > 12 mg/dl had a sensitivity of 88.46 % (23 patients, P = 0.1234NS) and it missed three patients all of whom developed local complications. It had a specificity of 48.86% (12 patients, P = 0.0031), which was significantly less than that of RBS. The major disadvantage was that 16 of the 28 mild cases were wrongly predicted as severe. White blood cell counts > 14.5 (x 103/dl) had a sensitivity of 61.54 % (16 patients, P = 0.0082) and it missed ten patients. It had a specificity of 75% (21 patients) and seven patients were wrongly predicted as severe. Pulse > 100/min had a sensitivity of 34.62%, (nine patients, P = 0.0019), and it missed 17 patients. It had a specificity of 85.71% (24 patients) and four patients were wrongly predicted as severe. On analyzing, the predictive value of different combinations of the four variables RBS > 150 mg/dl + BUN > 12 mg/dl was found to have the maximum sensitivity of 76.92 % (20 patients, P = 0.0482) and specificity of 85.71% (24 patients). The sensitivity of this combination was significantly lower than that of Biliary Ranson. All other combinations had a sensitivity of <60%. The comparison of prognostic value of all these factors is shown in [Table - 3]. Discussion In spite of the various experimental interventional studies in acute pancreatitis, an accurate and a simplified predictor of the outcome of acute pancreatitis still eludes us. Prediction of the severity of acute pancreatitis is important because those with severe diseases could be selected for, and may be benefited by prompt intensive treatment. Those with mild diseases could be spared from costly and invasive protocol.[6] Ranson et al.[1] identified 11 objective factors to determine the severity in patients with acute pancreatitis. Because 69% of these cases were associated with alcohol, Ranson[5] revised the criteria for patients with biliary pancreatitis. Imrie et al[7] gave a modification of the Ranson's prognostic scoring system and reduced the factors to nine. Osborne et al[8] modified Imrie criteria by omitting the age factor. Blamey et al[2] further modified Imire criteria by including the age factor and omitting transaminase. Acute physiology and chronic health evaluation II system of disease severity assessment was given by Knaus et al.[3] There were a number of disadvantages associated with the scoring systems mentioned in the preceding text. Neoptolemos et al[9] suggested that the number of patients with gallstone pancreatitis in the study of Ranson in 1982 was inadequate (70% were again of alcoholic origin) to provide an accurate prognostic scoring system and APACHE-II is disadvantageous in routine use because of its complexity. Mc Mahon et al.[10] suggested that the initial clinical assessment could not correctly predict the severity of the attack. He further reported that by 48 h the accuracy of clinical assessment to predict severity improved up to 83%, which was equivalent to that of multiple scoring systems. Some authorities believe that multiple scoring systems have too many values to be memorized, need 48 h for assessment thereby leading to the wastage of most crucial, investigative and interventional time, and parameters may be influenced by treatment in 48 h.[11] Others have previously reported the value of simplified prognostic criteria for acute pancreatitis. High plasma glucose is reflection of the severity of damage to islet cells.[12] Seligson et al[13] showed that acute pancreatitis was associated with deficient B-cell function and decreased glucose tolerance. These studies suggest that higher RBS levels may indicate a more severe damage to the pancreas and that RBS could be used as a prognostic indicator. Jacobs et al[14] demonstrated that admission urea level exceeding 8.6 mmol/l was associated with a mortality rate of 49%. Some authors believed that an elevated urea level indicates hypoperfusion, which may lead to the development of pancreatic necrosis.[15] Another study showed that an elevated serum urea level could be a reflection of poor renal reserve, hypovolemia, or gastrointestinal bleeding making these patients more susceptible to complications.[16] In the study of Fan et al[17] the sensitivity and specificity of the combined serum glucose > 11.0 mmol/l (200 mg/dl) and/or BUN > 7.4 mmol/l (20 mg/dl) criteria was 75.0 and 80.3%, respectively and was comparable to the Imrie scoring system. Fan et al[18] later validated their findings of the earlier study by using the same cut-off values of serum urea/plasma glucose criteria. The sensitivity was 79% and specificity was 67%, which were comparable to APACHE-II, Ransons, and Imrie scoring system. These findings indicate that higher serum glucose and blood urea levels correlate with the severity of pancreatic insult and that these may be used as a prognostic criteria. Meek et al[4] studied the prognostic value of simple admission criteria (WBC > 14.5 x 103/dl; BUN > 12 mg/dl; RBS > 150 mg/dl; pulse > 100/min) and compared them with APACHE-II > 5, Biliary Ranson 3, and modified Imrie > 3. They demonstrated that admission value of RBS > 150 mg/dl had a sensitivity of 82% and a specificity of 85% in patients without diabetes, and it was the best single predictor of severity. They also added that it was less cumbersome than scoring systems and allowed immediate triage to appropriate level of hospital care. In this study both RBS > 150 mg/dl and BUN > 12 mg/dl had sensitivity of 88.46%, which was comparable to APACHE-II > 5, Biliary Ranson > 3, and modified Imrie > 3. BUN > 12 mg/dl had the disadvantage of very low specificity (42.86%), being significantly lower than that of RBS > 150 ml/dl (78.57%), which led onto a large number of mild attacks to be graded as severe. A level of RBS > 150 mg/dl at admission can act as an indicator to the clinician of the high probability of the patient to develop severe complications and demands a more careful monitoring. However, this does not indicate any change in the clinical guidelines for the initial management of acute pancreatitis. Also, repeated clinical examinations and monitoring of baseline parameters in the initial 72 h should be done because it enables the clinician to identify the patients who develop complications. This study validates the findings of Meek et al[4] and we can conclude that RBS > 150 mg/dl can be used as a simplified prognostic indicator as it is simple to be used in both rural and urban settings, is readily available at admission, and allows rapid assessment of severity. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05037t1.jpg] [is05037t2.jpg] [is05037t3.jpg] |
| |||||||||

{kind=link}
{kind=link}