 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 67, No. 3, May-June, 2005, pp. 140-142 Original Article Morphological spectrum of gallstone disease in 1100 cholecystectomies in North India Mohan H, Punia RP S, Dhawan SB, Ahal S, Sekhon MS Departments of Pathology and Surgery, Government Medical
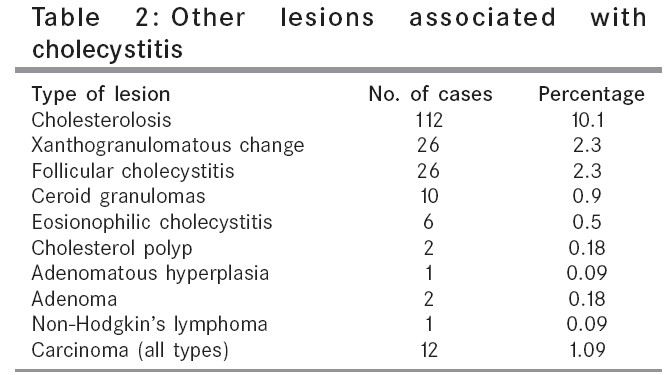
College and Hospital, Chandigarh, India Code Number: is05038 Abstract BACKGROUND: Gallstones are a major cause of morbidity and mortality throughout the world. In India, they are seven times more common in the North as compared to the South.AIMS: To study the morphological spectrum of gallstone disease in the stone- belt of India, and to understand its probable etiopathogenesis. MATERIALS AND METHODS: Morphological spectrum of gallstone disease was studied in 1100 cholecystectomies over a period of 3 years in the past. RESULTS: There was a preponderance of females (M: F ratio 1: 6.4). The age of the patients varied from 10 to 90 years with maximum number of cases between 31 and 40 years of age. On morphological analysis, gallstones were of mixed type in 686 cases (62.3%), pigment type in 34 cases (3.2%), cholesterol type in 182 cases (17.3%), and combined type in 148 cases (14%). Other lesions associated with chronic cholecystitis were cholesterolosis in 112 cases (10.1%), xanthogranulomatous cholecystitis in 26 cases (2.3%), follicular cholecystitis in 26 cases (2.3%), ceroid granulomas in ten cases (0.9%), eosinophilic cholecystitis in six cases (0.5%), and carcinoma in 12 cases (1.09%). Maximum number of carcinomas were associated with pigment stones, that is, 7 out of 12 cases (58.3%). CONCLUSIONS: The morphological spectrum of gallstone disease in this stone-belt of India will certainly contribute to understand its etiopathogenesis, and hence prevention. However, further studies on the biochemical composition of stones and their association with morphological changes are required to clarify the etiopathogenesis. Keywords: Carcinoma, cholecystitis, cholelithiasis, cholesterolosis, gallstones Gallstones are a major cause of morbidity and mortality throughout the world.[1] At least 10% adults have gallstones.[2],[3] The prevalence varies with age, sex, and ethnic group.[1] Most patients are unaware of the disease and remain asymptomatic for life. Only a small percentage develop symptoms necessitating treatment.[4] Nowadays, laparoscopic cholecystectomy is the treatment of choice in most patients.[5] Gallstones vary in their composition, a majority being cholesterol stones (80%), and the remaining being mixed, combined, and pigmented.[6] The diseased gallbladder, in association with gallstones show variety of morphologic changes ranging from inflammation to malignancy. The present study is aimed at clinicopathologic analysis of gallstone disease in this part of the country. Materials and Methods The retrospective study was conducted on 1100 cholecystectomies performed at our hospital over a period of 3 years in the past. Clinical details and pathological data were retrieved from the records. The cholecystectomy specimens that were received were fixed in 10% formalin. The findings on gross examination were noted, and the stones recovered from the gallbladder were classified on the basis of their morphology [Table - 1]; however, stones were not analyzed by chemical examination. Two sections were taken from each gallbladder for paraffin blocks and were examined after staining with hematoxylin and eosin staining. Microscopic examination was done to assess the type of inflammatory infiltrate, presence of fibrosis, cholesterolosis, metaplasia, tumor, or tumor-like lesion. Statistical analysis Results The age of patients varied from 10 to 90 years with maximum number of patients (316/1100, 28.7%) being between 31 and 40 years. There were 148 males and 952 females with M: F ratio of 1: 6.4. On the basis of morphological analysis it was found that a maximum percentage of cases had mixed type of gallstones (686 cases, 62.3%), followed in decreasing frequency by cholesterol (182 cases, 17.3%), combined (148 cases, 14%), and pigment type (34 cases, 3.2%) [Table - 1]. In our study, there were two children and both had cholesterol stones. In 50 cases (4.5%), there were no gallstones, but on histological examination all these cases too showed changes of chronic cholecystitis. In addition, histological examination of gallbladder showed other variants of cholecystitis [Table - 2]. Association of the type of gallstones with cholesterolosis, xanthogranulomatous change, and carcinoma showed that cholesterolosis was associated not only with cholesterol stones but also with mixed stones. Xanthogranulomatous change was associated most often with mixed gallstones (19/26 cases, 73%). In two patients, there was adenoma with gallstones. In one patient, the gallbladder wall showed lymphomatous infiltration diagnosed incidentally. Carcinoma of the gallbladder was seen in 12 cases (1.09%) and it was associated most often with pigment stones (7/12 cases, 58.3%) [Table - 3]. Statistical analysis revealed significant association of cholesterolosis with cholesterol stones ( P < 0.01). However, association of cholestrolosis with mixed and combined stones was significantly low. There was no significant association of xanthogranulomatous cholecystitis with type of stone. Carcinoma gallbladder showed significant association with pigment stones ( P < 0.01). Discussion Gallstones are frequently found at autopsy in subjects who have apparently gone through life without symptoms of their gallstone disease, indicating that many people have gallstones without ever becoming aware of them. The estimated prevalence of gallstone disease in India has been reported as 2% to 29%.[7],[8] In India, this disease is seven times more common in the North (stone belt) than in South India.[9] Dietary differences in the two regions are suspected to be responsible for the difference in the prevalence rate.[10] The average age of these patients in India, is a decade younger than those in the West.[11] The maximum number of patients in this study were in the third decade of their life (316 cases, 28.7%). Studies have shown an increase in the prevalence of gallstones with age probably because of decrease in activity of cholesterol á reductase, and increase in activity of HMG CoA reductase resulting in increased cholesterol secretion and saturation of bile.[12] Male to female ratio in this study was 1: 6.4. Other studies have also shown predominance of females among patients with gallstone disease. In fact, female sex hormones and sedentary habits of most women in India exposes them to factors that possibly promote the formation of gallstones.[11],[13],[14] In our series, 62.3%, 17.3%, 14.1%, and 3.2% were mixed, cholesterol, combined, and pigment stones, respectively. Other studies have also reported similar incidence of the type of gallstones; however, literature reports, from Chennai were in contrast to our study where majority of gallstones are pigment stones and the remaining are mixed and cholesterol type.[5],[9],[15] In the pathological findings, cholesterolosis was the commonest change noted (112 cases, 10.1%). Cholesterolosis was present in 26.3% of cases with cholesterol cholelithiasis, and 6.8% of cases with mixed cholelithiasis. Chronic xanthogranulomatous cholecystitis was observed in 26 cases (2.3%). These cases usually present with increased wall thickness and mimic carcinoma on gross. Awareness of this entity and careful microscopic examination helps in diagnosis. Chronic follicular cholecystitis was noted in 26 cases (2.3%). This entity is considered as variant of chronic cholecystitis and represent lymphoid hyperplasia in wall of gallbladder. Other morphological lesions were rare. Carcinoma of gallbladder is a rare but lethal disease. In the present study, there were only 12 cases (1.09%). Different studies have reported different incidences ranging from 1% to 12.4%.[16],[17] This difference is because carcinoma gallbladder usually presents as an inoperable stage as a result of infiltration into the liver and therefore surgery is not undertaken. In our study, 100% patients with cancer had gallstones. Maximum number of patients with cancer had pigment stones. Laparoscopic cholecystectomy, introduced in 1987 by Mouret, and then used in 1988 by Du Bois et al., is the treatment of choice.[6] However, major challenge is medical prevention of gallstone formation in susceptible individuals, although cholecystectomy remains the cornerstone of treatment. Studying the morphological spectrum of gallstone disease in this stone-belt of India will certainly contribute to understand its etiopathogenesis and hence prevention. However, further studies on biochemical composition of stones and their association with morphological changes are required to clarify the etiopathogenesis. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05038t3.jpg] [is05038t2.jpg] [is05038t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}