 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 67, No. 3, May-June, 2005, pp. 143-144 Case Reports Pyonephrotic kidney-An initial manifestation of cystic renal cell carcinoma Singh Iqbal, Ansari MS Department of Urology, All India Institute of Medical
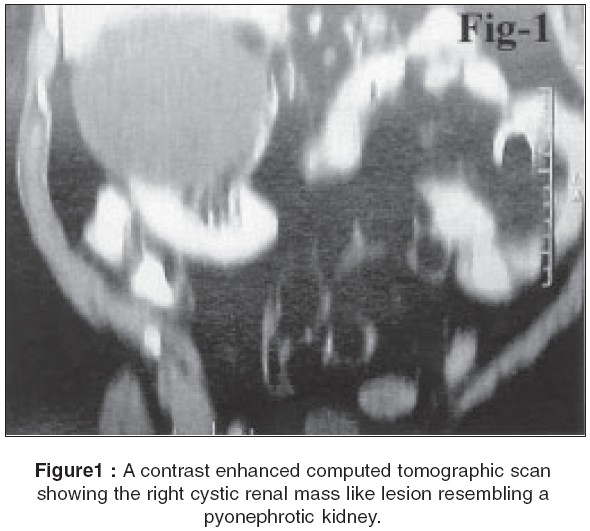
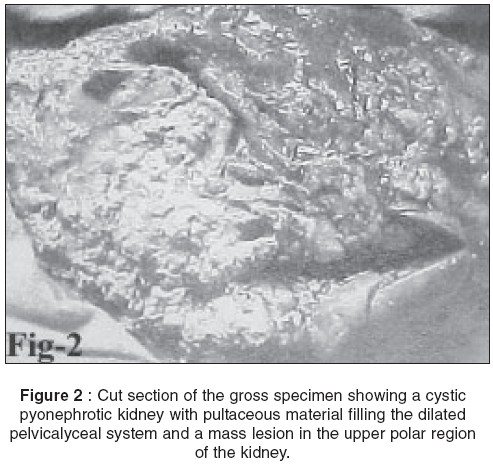
Sciences, New Delhi, India Code Number: is05039 Abstract We describe an unusual and rare case of pyonephrotic kidney in a middle-aged man that ultimately turned out to be a concealed case of an underlying cystic renal cell carcinoma. In the present case an underlying renal cancer was probably the cause of cystic degeneration of the renal pelvicaylceal system complicated secondarily by pyonephrosis which was the initial presenting manifestation. We describe the second such unusual case to be reported in the English literature. We have described diagnostic problems and the underlying clinical manifestation of such a rare case.Keywords: Renal cell carcinoma, renal cancer, cystic renal tumors, pyonephrosis CASE REPORT A 45-year-old man presented with complaints of dull aching right flank pain for the past ten days accompanied with fever. There was no history of dysuria, UTI or any other voiding symptoms. The local examination was unremarkable apart from mild tenderness in the right flank on deep palpation. The urine analysis and blood renal function tests were within normal limits. An ultrasound of the KUB region revealed an upper polar right renal cyst measuring about 5x6 cms with a normal opposite renal unit. The IVP confirmed a non-visualized right kidney. A contrast enhanced computed tomography scan confirmed a 6x7 cms cystic mass lesion involving the upper and mid polar region of the right kidney suggestive of a minimally complicated Type-3 renal cyst. [Figure - 1] After 4 days of parenteral antibiotics, which failed to improve his condition, a decision to proceed to right nephrectomy was taken. A percutaneous nephrostomy was considered but was not done as there was a lurking suspicion of a renal tumor due to the suspicious nature of the renal cyst (Bosniak type-3). The gross cut specimen of the kidney revealed a pyonephrotic kidney with soft pultaceous fluffy material and purulent fluid occupying the cystic spaces of the kidney and a mass lesion in the upper and mid pole of the kidney [Figure - 2]. Based on this diagnosis of a right pyonephrotic kidney was made. The histopathology was reported as right cystic renal cell carcinoma (clear cell type). The patient is doing fine on a further follow up of six months with no evidence of any metatstatic disease.DISCUSSION Renal cell carcinoma has been rightly called the internists tumor and described as one of the greatest mimicker in medicine. Renal cancer is known to be confused with lesions such as emphysematous pyelonephritis[1], xanthogranulomatous pyelonephritis[2], pyonephrosis[3], renal abscesses[3] and differentiating them from renal cancer is often difficult. In the present case also the initial clinical manifestation was strongly suggestive of acute pyelonephritis culminating in pyonephrosis that could not be differentiated form a renal cancer (though it's presence could not be ruled out due to the suspicious nature of the renal cyst). It is possible that this had occurred as a complication of long standing cystic renal cell carcinoma. Whilst cystic degeneration is not uncommon in renal cell carcinoma (as up to 15% of renal cancers may be radiologically cystic)[4], rather it was the detection of pyonephrosis that was a rare initial presenting complication in the present case which had concealed the underlying cause. The cystic spaces were probably the result of an obstructing renal cell carcinoma leading to a ballooned out pelvicalyceal system, which got secondary complicated by pyonephrosis. We can only speculate as to the genesis of pyonephrosis. The origin of the purulent fluid may have been due to either a sympathetic effusion from the renal cancer cells or due to a loculated fluid collection, which was secondarily infected. Whether this was due to a pre-existing renal cystic lesion that may have developed a renal cancer is also debatable. Thus while the diagnosis of pyelonephritis and pyonephrosis is comparatively easy, however ascertaining the source of obstruction and or infection is often complex. This is of vital importance so as to plan appropriate curative therapeutic strategies. In the present case this turned out be a concomitant cystic renal cancer. Renal cancer may rarely spread insidiously to involve the calyces and pelvic infundibulae resulting in extensive renal destruction with pyonephrosis. This may not be detected on a routine IVP due to their late presentation with a non-functioning renal unit as had occurred in the present case. A CT scan can only define the renal cyst in greater detail, but cannot always pinpoint a renal cancer as this may be just a subtle lesion on the renal septae and cysts and surgical sampling/resection by nephrectomy may the only way to definitely rule out renal cancer.[5] To the best of our knowledge this is the second[3] such case to be reported in the English literature. We reported the present case to alert the treating surgeon and urologist to the fact that renal cancers may at times mimic a pyonephrotic kidney and differentiation from each other is not always possible preoperatively despite the availability of wide investigative armamentaria. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05039f1.jpg] [is05039f2.jpg] |
| |||||||||

{kind=link}
{kind=link}