 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 67, No. 3, May-June, 2005, pp. 147-149 Case Reports Mediastinal and Retro-orbital emphysema following an uncomplicated endoscopic sphincterotomy M. Aydin, E. Kisli1, E. Ozgoren1, O. Soylemez1, M. Baser1, A. Aslaner Department of General Surgery, Düzce School of Medicine, Abant izzet
Baysal University, Düzce, Turkey and 1Department of
General Surgery, School of Medicine, Yüzüncü Yýl
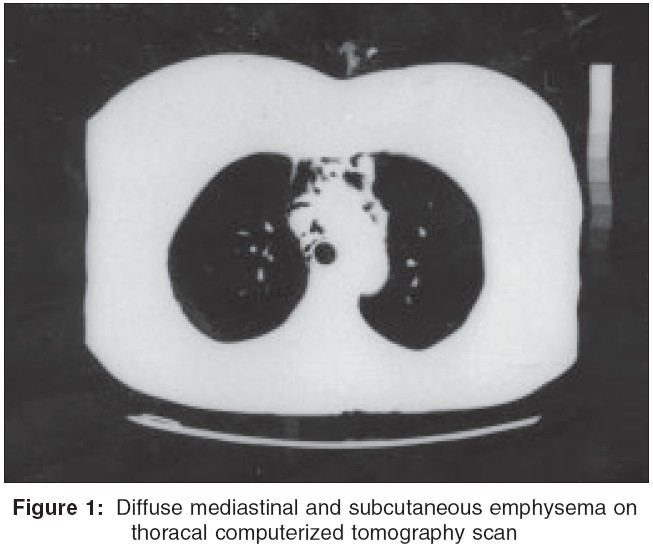
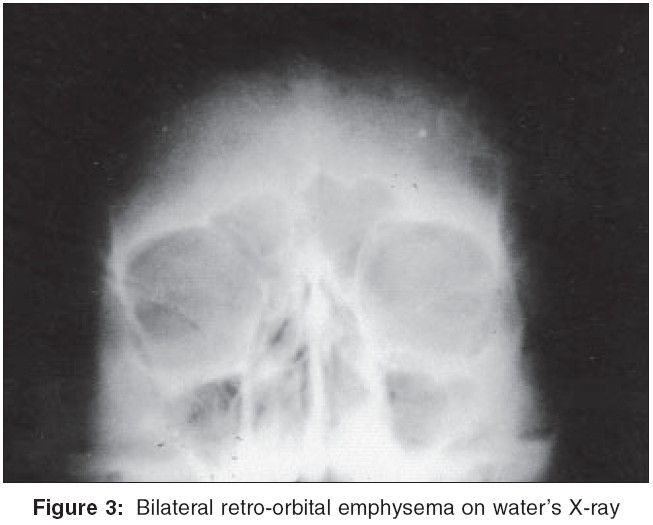
University, Van, Turkey. Code Number: is05041 Abstract We report a case of mediastinal and bilateral retro-orbital emphysema following an uncomplicated endoscopic sphincterotomy. The concurrent presence of these complications following endoscopic retrograde cholangiopancreatography is rare. The simultaneous occurrence of these two complications in the same patient has not been previously reported in the literature. Furthermore, we define the first case of mediastinal and bilateral retro-orbital emphysema following endoscopic sphincterotomy.Keywords: Emphysema for emphesema, Sphincterotomy for sphincetrotomy Endoscopic retrograde cholangiopancreatography (ERCP) is one of the most effective methods able to use in the diagnosis and treatment of biliary tract, pancreatic duct, and periampullar diseases. Recently, its popularity is getting higher in lithotripsy, endoprosthesis placement, stone extraction, and sphincterotomy.[1],[2] However, life-threatening complications could sometimes occur. In this case, a rare complication of ERCP was investigated in the review of literature. CASE HISTORY A 63-year-old woman was admitted to our clinic complaining of abdominal pain, nausea, and vomiting. She had cholecystectomy 7 years ago. Laboratory investigations were in normal ranges. Ultrasonography (US) revealed a stone 10 millimeters (mm) in size in distal choledoc and the diameter of the choledoc was 15 mm. The patient was scheduled for ERCP (Pentax FD-34P). During ERCP, papilla of Vater was normal. Choledoc was catheterized following papillotomy. Two opacified stones 7 and 4 mm in size, which were in distal choledochus, were determined on cholangiography and the diameter of the choledoc measured 2 cm. The stones were extracted by balloon following sphincterotomy. There were no anatomical abnormalities. Endoscopic retrograde cholangiopancreatography lasted 90 min and later a direct abdominal graphy was taken and free air was not observed. We observed swelling and crepitation all over the face, more manifested on bilateral periorbital region after the second hour of ERCP. There was no evidence of peritonitis on physical examination. Blood pressure and pulse were normal. Diffuse mediastinal and subcutaneous emphysema were detected on thoracal computerized tomography (CT) scan [Figure - 1]. Emphysematous findings were established in the lower cervical region on CT scan [Figure - 2]. Bilateral retro-orbital emphysema was detected on water's X-ray image [Figure - 3]. Nasogastric decompression and prophylactic antibiotheraphy were begun. On the 48th hour of ERCP, clinical findings returned to normal ranges and all the symptoms disappeared on the fourth day after ERCP. Discussion Endoscopic retrograde cholangiopancreatography is one of the most effective methods to use in the diagnosis and treatment of biliary tract, pancreatic duct and periampullar diseases. Recently, it is gaining popularity in lithotripsy, endoprosthesis placement, stone extraction and sphincterotomy.[1],[2] In exception of general endoscopic complications as premedication reaction and cardiopulmonary problems, the complication rate dependant on ERCP is 2-7%.[2],[3] Most frequently, complications depend on pancreaticobiliary cannulation.[2] After ERCP and sphincterotomy, the rate of major complications such as pancreatitis, bleeding, cholangitis, fever, hepatic abscess, sepsis, and perforation is about 10%. Mortality rate is about 0.1% and perforation due to ERCP is 1.5-2% and it is usually diagnosed during the procedure.[3],[4] Zissin et al. and Guitron et al. report that retroduodenal perforation could be seen at a rate of 1.13% and dependant on that retroperitoneal free air could be seen on CT scan.[5],[6] In a study, duodenal pneumotosis that developed after sphincterotomy performed with ERCP was reported.[7] Gya et al. have reported right pneumothorax and subcutaneous emphysema after sphincterotomy in a patient who had ERCP.[8] Retroperitoneal perforation can occur in different ways.[3] Known symptoms and findings are upper abdominal pain spreading toward back, fever, mass on right iliac fossa and dye-like bilirubine as Gray Turner sign on flank although serum amylase level is normal. Colemont et al. have reviewed unilateral periorbital emphysema on early term in a case of ERCP and explained this issue with anatomical connections of the neck mediastinal and retroperitoneum after retroduodenal perforation.[9] Complications such as pneumoperitoneum, pneumomediastinum, and subcutaneous emphysema were reviewed during investigation of upper gastrointestinal tract with fiber optic endoscopy,[10] but bilateral periorbital emphysema which has occurred after pneumomediastinum, subcutaneous emphysema and pneumoperitoneum that developed after duodenal perforation secondary to endoscopic papillotomy was not found in a search of the literature. Gya et al. have reviewed a case in which periorbital emphysema with pneumothorax occurred unilaterally.[8] Complications such as bilateral periorbital and cervical subcutaneous emphysema without pneumothorax that occurred in our case, has coincided in two patients on searching the literature. This pathophysiologic situation is explained with a small perforation, which was occurred on the posterior duodenal wall and the gas diffused to perioesophageal area through this retroperitoneal diaphragmatic space and then spread to trachea and visceral areas, which cover the esophagus throughout the deep neck fascia, which is connected with the mediastinum. It causes periorbital and cervical subcutaneous emphysema. Mediastinal, cervical, and periorbital emphysema and also pneumothorax after retroduodenal perforation are unusual; however, because of the abnormalities of anatomical structures that are connected with each other as mentioned above and elevated gas pressure during ERCP, it could be developed easily and spread to other areas. Finally, for preventing complications like these, we recommend that needle papillotomy should be used more carefully especially in difficult and long ERCP procedures. Known complications of ERCP reviewed in textbooks and the literature until today is mediastinal, cervical, and subcutaneous emphysema in two cases and periorbital emphysema in one case. These complications can develop after a long and complicated ERCP. In this case, the patient did not have an acute abdomen and the vital parameters stayed stabile, hence treatment should be conservative without considering an urgent laparotomy. We define the first case of mediastinal and bilateral retro-orbital emphysema following endoscopic sphincterotomy. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05041f3.jpg] [is05041f2.jpg] [is05041f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}