 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 67, No. 3, May-June, 2005, pp. 152-155 Case Reports Leiomyosarcoma of the inferior vena cava: An uncommon cause of inferior vena caval obstruction Swaminathan TS, Srinivasaraman Govindarajan, Anand T, Senthilkumar AR Barnard Institute of Radiology, Madras Medical College,
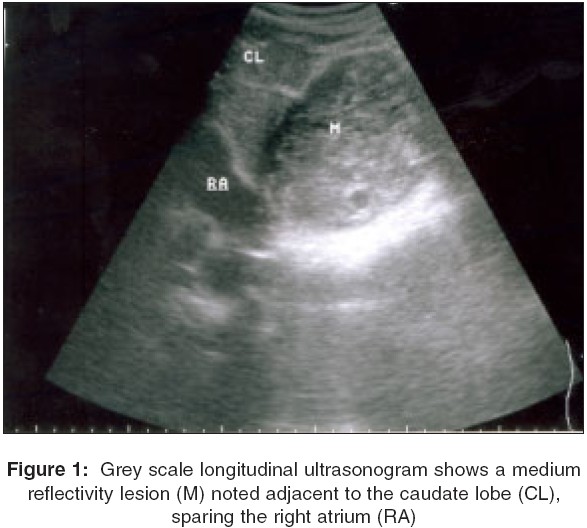
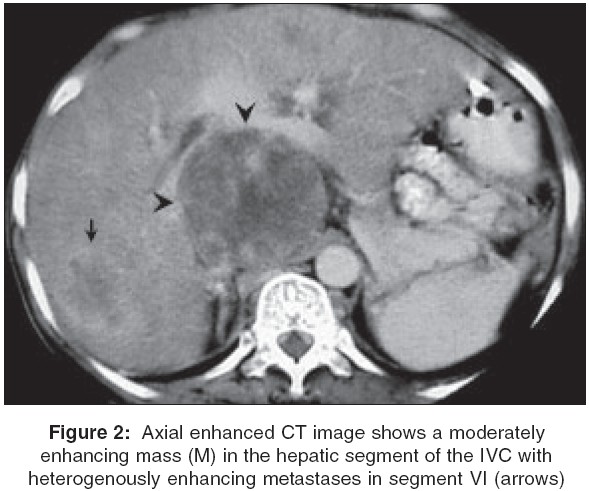
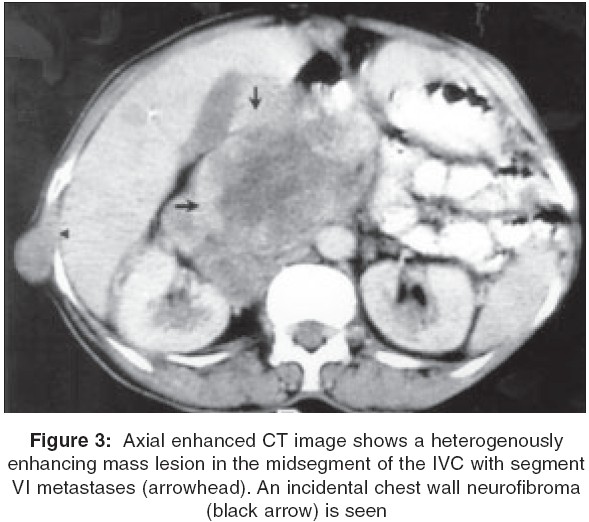
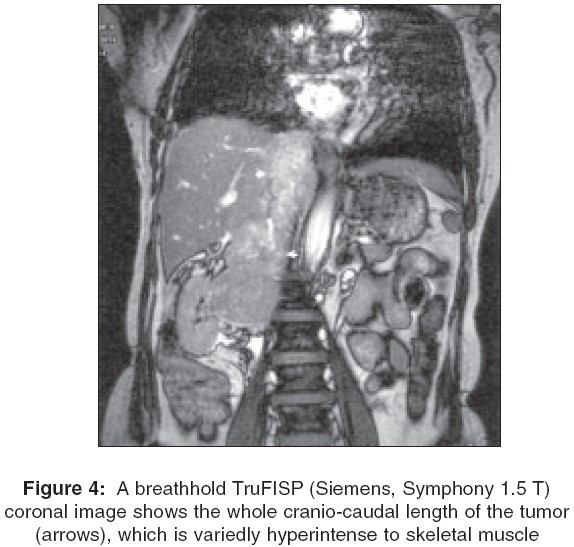
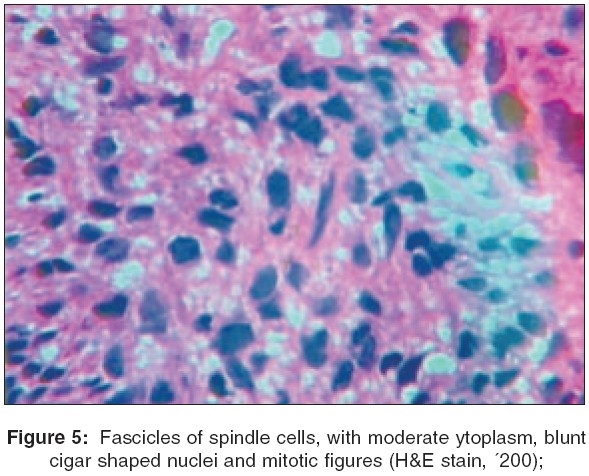
Chennai, India Code Number: is05043 Abstract Venous leiomyosarcomas are rare neoplasms usually afflicting the inferior vena cava. They usually present with abdominal pain, and an abdominal mass with features of IVC obstruction. Early and accurate diagnosis is essential, because radical surgery offers the only hope of prolonged survival. Imaging combined with guided biopsies forms the mainstay of reliable presurgical diagnosis. We describe a 48-year-old woman with leiomyosarcoma of the hepatic segment of the IVC, who presented with features of IVC obstruction. The imaging features of the tumor are described with a review of the current literature.Keywords: Inferior vena caval obstruction, inferior vena cava, Leiomyosarcoma Case history A 48-year-old woman presented with gross distension of the abdomen and swelling of both lower limbs for three months. Examination revealed an asthenic patient with bilateral pitting pedal edema, abdominal distension, dilated anterior abdominal wall veins and a nontender, ill-defined mass in the epigastric region. Ultrasound revealed a large, elongated lesion of medium reflectivity in the region of the IVC, adjacent to hepatic segment I [Figure - 1] . Caudally, the lesion extended just below the renal veins, which appeared spared. The distal IVC appeared rounded, as against the normal slightly flattened shape indicating proximal obstruction. Cranially, the lesion extended till the diaphragmatic caval hiatus, sparing the right atrium. The abdominal aorta was slightly displaced to the left by the lesion. A small rounded lesion of reduced reflectivity was noted in hepatic segment VI. Features of IVC obstruction and collateral formation, with preserved hepatic venous flow, were obtained with triplex doppler imaging. An enhanced CT revealed a large moderately enhancing hypodense lesion of the hepatic segment of the IVC [Figure - 2] and [Figure - 3]. The interface between the liver and the lesion was relatively well defined. Caudal extension below the renal veins, dilatation of the distal IVC and sparing of the renal veins were observed. Collateral formation, indicating gradual obstruction, was manifest as dilatation of the azygos, inferior and superior epigastric and paravertebral veins. MRI revealed a large well-defined mass in the hepatic segment of IVC, exhibiting heterogenous hypointense signals in T1 and hyperintense signals in T2 sequences with patchy areas of necrosis within [Figure - 4]. Signs of IVC obstruction including anterior abdominal, peritoneal and retroperitoneal collaterals were observed. A percutaneous ultrasound-guided biopsy of the tumor revealed interweaving fascicles of spindle cells with moderate eosinophilic cytoplasm, blunt-ended cigar-shaped nuclei with stippled chromatin and inconspicuous nucleoli [Figure - 5] . Occasional large pleomorphic cells were noted. Averages of eight mitotic figures per ten high-powered fields were found. An ultrasound-guided biopsy of the hepatic segment VI lesion yielded similar histology, indicating hepatic spread. Discussion Leiomyosarcomas are mesenchymal tumors usually afflicting the retroperitoneum or uterus. In the vasculature, the venous system is commonly affected. Half of all venous leiomyosarcomas occur in the IVC and are the most common tumors of the IVC, usually found in middle-aged women, afflicting the midsegment.[1] Leiomyosarcomas arise from vascular smooth muscle and may exhibit an intrinsic or extrinsic or commonly a combined growth pattern. Histology reveals blunt-ended, variably pleomorphic spindle cells with cigar-shaped nuclei, arranged in fascicles.[2] Immunohistochemistry is usually positive for muscle-specific actins and often, but not invariably, desmin. The symptomatology relates to tumor site and extent.[3] At their frequent location, in the mid segment, the tumors may present with IVC obstruction or may extend into the renal veins, causing the nephrotic syndrome. Complete obstruction and the Budd Chiari syndrome are well-documented results, usually with hepatic segment tumors. Right atrial extension can occur resulting in atrial arrhythmias. Associated thrombosis is frequent and embolization not unknown. Tumors of the lower segment may present late. While local invasion is rare, approximately 20% of tumors have metastasized at presentation, commonly hematogenously, to liver and lung, although lymphatic spread is not altogether unknown.[3] Computed tomography and Magnetic Resonance Imaging are considered the imaging modalities of choice.[4],[5] CT reveals moderately enhancing hypodense lesions with areas of necrosis, expanding and extending along the course of the IVC.[6] MRI reveals the intraluminal tumors to be isointense to hypointense on the unenhanced T1 images and heterogenously hyperintense on the T2 weighted image. Administration of intravenous gadolinium chelates usually results in moderate enhancement, reflecting, in part, the vascular nature of these tumors. As with CT, extension into the right atrium or the hepatic and renal veins can be analyzed.[7] Ultrasound reveals these tumors to be predominantly mixed in echogenicity, with the necrotic areas being especially echopenic.[8] When combined with doppler studies, the hemodynamics of the caval obstruction and renal vein thrombosis can be accurately assessed. Further, bland thrombus may be differentiated from tumor by the presence of vascularity in the latter, especially with power doppler studies. Cavography, although currently uncommonly performed for diagnosis, depicts the collateral pathways in exquisite detail and may provide useful information for planning venous reconstructions.[9] Other tumors, notably renal cell carcinomas, are particularly prone to extension into the inferior vena cava. The presence of an associated renal mass usually permits differentiation. A bland thrombus, often the usual cause of an IVC obstruction, seldom attains the large size that most leiomyosarcomas do. The lack of contrast enhancement, the relative homogeneity of the lesion and signals suggestive of paramagnetic products of hemoglobin degradation on MRI usually allow distinction between the two. Differentiation between a mixed type of Leiomyosarcoma and a retroperitoneal sarcoma secondarily invading the inferior vena cava may be difficult. A percutaneous transluminal biopsy technique has been described[3] and it is now often possible to arrive at a definite preoperative diagnosis. Surgery forms the mainstay of treatment; however, the tumors afflicting the hepatic segment are often unresectable. Imaging, in many of these situations, allows assessment of the degree of resectability[1] of these tumors. Tumors of the mid segment are reported to have the best prognosis with a 50% survival rate at ten years.[1] Hepatic segment tumors, presence of IVC obstruction, large size of the tumor, high mitotic index and presence of associated thrombus are considered poor prognostic indicators.[10] Conclusion Leiomyosarcoma of the inferior vena cava (IVC) must be considered in the list of differentials of a mass lesion adjacent to hepatic segment I with signs of IVC obstruction. A renal cell carcinoma or an adrenal carcinoma with extension into the IVC, angiosarcoma of the IVC, a bland thrombus and a retroperitoneal sarcoma invading the IVC are the other lesions occurring at this site. An accurate interpretation of the clinical and imaging findings usually allows accurate diagnosis.References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05043f5.jpg] [is05043f1.jpg] [is05043f4.jpg] [is05043f3.jpg] [is05043f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}