 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
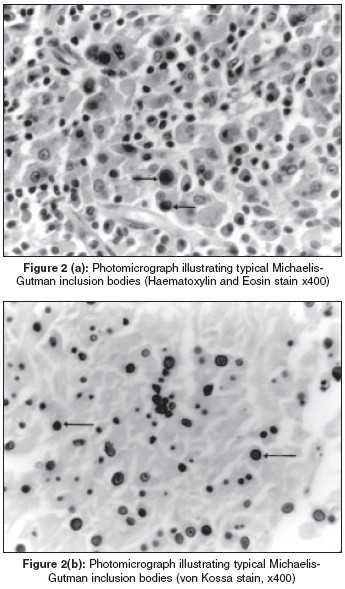
Indian Journal of Surgery, Vol. 67, No. 3, May-June, 2005, pp. 156-158 Case Reports Malakoplakia of the Gallbladder Sengupta Shomik, Buchanan Malcolm, Danne Peter Departments of Surgery and Anatomical pathology, Royal Melbourne Hospital and The University of Melbourne, Parkville, Victoria, Australia Code Number: is05044 Abstract Malakoplakia, a rare inflammatory condition usually occurring in the urinary tract, may occasionally be seen in other viscera, including the gall bladder. We describe one of the few cases of malakoplakia in the gall bladder, wherein, due to diagnostic confusion with carcinoma as well as operative difficulty, open cholecystectomy was necessitated. Malakoplakia of the gall bladder may be seen rarely, and then only incidentally, but needs to be kept in mind as a potential differential diagnosis for carcinoma and granulomatous cholecystitis.Keywords: Carcinoma, cholecystectomy, cholecystitis, gall bladder, granulomatous cholecystitis, malakoplakia, Michaelis-Gutman bodies Introduction The histopathology of cholecystectomy specimens is usually predictable, and often given only cursory attention to exclude incidental malignancy. We present an incidental histological finding in the gall bladder of the rare lesion of malakoplakia, and discuss the clinical significance of this finding as a mimic of carcinoma of the gall bladder.Case Report An 84-year-old man with multiple medical problems, including gout, coronary heart disease and hypothyroidism, presented to us with upper abdominal pain and fever, and was diagnosed as suffering from acute cholecystitis. Imaging findings at the time were unremarkable, and as he improved with conservative management, he was placed on the waiting list for elective cholecystectomy. While waiting for surgery, he presented some months later with obstructive jaundice, and was treated successfully by endoscopic sphincterotomy and stone extraction. A further three months later he underwent cholecystectomy. The procedure was begun laparoscopically, but needed to be converted to an open cholecystectomy because the gall bladder was friable, thickened and adherent, which made it difficult to manipulate and raised intra-operative concerns regarding possible malignancy. A frozen section of the gall bladder wall was performed, but was negative for malignancy. Paraffin sections revealed chronic cholecystitis [Figure - 1], with sheets of histiocytes containing intracytoplasmic inclusion bodies [Figure - 2]a) which stained positively with the von Kossa stain [Figure - 2]b). The patient suffered postoperative transient cerebral ischaemic events and respiratory problems, but after a prolonged hospitalisation and rehabilitation, was discharged home.Discussion Malakoplakia is a rare entity, usually found in the urinary tract[1] but described in a wide range of tissues.[1],[2],[3] Its occurrence in the gall bladder has been reported rarely. [4],[5],[6] Malakoplakia outside the genito-urinary tract is often an incidental diagnosis,[2] but may present as chronic infection or a mass suspicious for malignancy.[1],[3] While malakoplakia is a benign pathological process, it may behave aggressively, particularly in the gastro-intestinal tract.[4] The intra-operative findings in this patient were suggestive of malignancy, and led to open conversion, which may have contributed to postoperative complications. In other reported cases, the suspicion of malignancy has also been raised by pre-operative imaging and led to the subsequent open surgical removal of the gall bladder.[4] Granulomatous cholecystitis can present in a manner similar to malakoplakia,[6],[7] and the two entities may form part of a spectrum of chronic inflammatory conditions.[4] Pathologically, the gross appearance of malakoplakia is of a soft yellowish mass.[1],[3],[4] Microscopically, malakoplakia is characterized by a mononuclear cell infiltration. The so-called Michaelis Gutman inclusion bodies [Figure - 2] seen in some of these cells are pathogonomonic. Michaelis Gutman bodies are discrete, lamellated structures 5-10 μm in diameter, which are thought to represent remnants of phagosomes mineralised by calcium and iron deposits. [1],[2],[3],[4] Surgical excision and antibiotic therapy form the mainstay of therapy against malakoplakia, although a variety of other treatments have been tried.[2] Cholecystectomy, with or without peri-operative antibiotics, is likely to be adequate treatment for malakoplakia of the gall bladder, although the small number of cases do not allow for a detailed assessment of therapeutic efficacy at this stage. The pathogenesis of malakoplakia is not proven, but it is thought to arise from chronic infection and a deficient lytic response by macrophages.[1],[4],[8]-[9] The preponderance of malakoplakia in the urinary tract and the colon, and its rarity in the gall bladder, may be explained by the fact that exposure to coliform organisms in the former sites is much more frequent.[1] Immunosuppression, thought to be another important pathogenetic factor in the development of malakoplakia,[4],[8] may have occurred in our patient as a result of his age and co-morbidities. It is hypothesised that the phagocytosis of precipitated bile constituents can also lead to the formation of the typical inclusion bodies.[5] Thus it is possible that delayed elective cholecystectomy, as undertaken in this instance, may predispose to this rare pathological entity because of persisting gram negative infection and bile crystallization in the gall bladder. Therefore it is prudent to manage cases of cholecystitis by early cholecystecomy where feasible. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05044f1.jpg] [is05044f2.jpg] |
| |||||||||

{kind=link}
{kind=link}