
|
Indian Journal of Surgery
Medknow Publications on behalf of Association of Surgeons of India
ISSN: 0972-2068
Vol. 67, Num. 4, 2005, pp. 189-194
|
Indian Journal of Surgery, Vol. 67, No. 4, July-August, 2005, pp. 189-194
Original Article
Patient selection for cholecystectomy based on oral fatty meal augmented cholescintigraphy in cases with chronic acalculous biliary pain: Is it really that reliable?
Chin KH., Sahlén AO, Farouk MO
Department of Surgery, Stoke Mandeville Hospital, Aylesbury, Buckinghamshire, UK
Correspondence Address:KH Chin, FRCS 17, Oriel Mews, Lamarsh Road, Oxford OX2 0LD, UK. E-mail: kianhchin@yahoo.com
Code Number: is05059
Abstract Background: Gallstones disease associated with biliary symptoms such as gallbladder dyspepsia (episgastric discomfort, flatulence, intermittent nausea with fat intolerance), and biliary colic (abdominal pain localised in the right upper quadrant) is commonly treated by cholecystectomy. In contrast, biliary symptoms in the absence of gallstones (acalculous biliary symptoms, ABS) often constitute a diagnostic and management challenge. Decision to recommend cholecystectomy to patients with ABS is sometimes based on abnormal cholescintigram, indicating biliary dyskinesia. Recently, the radiological protocol has changed from using intravenous stimulant to oral fatty meal to augment gallbladder contraction.
Objectives: To determine the long-term outcome of patients with ABS who underwent cholecystectomy based on abnormal cholescintigraphy using a new radiological protocol of oral fatty meal augmentation of the gallbladder.
Methods and Statistical analysis: A retrospective study of cholecystectomy was undertaken of all patients with ABS who were investigated with a fatty meal-augmented hepatic iminodiacetic acid (HIDA) scans between 1998 and 2001. Their case notes were reviewed. Pearson chi-squared test (SPSS Version 10.0.7 standard Version. SPSS incorporated 1989-1999) was used to analyse the relation between various parameters.
Results: Overall, 43 patients had HIDA scans. About 37 out of 43 (86%) patients had abnormal cholescintigrams, but only 25 were recommended surgery. Four patients were excluded owing to cholelithiasis. Sixteen patients (64%) were considered cured 6 weeks later. However, nine (36%) patients failed to improve with surgery after an average follow up of 33 weeks. Out of the 12 patients with abnormal HIDA scans who were managed conservatively, 5 (42%) recovered spontaneously, and 7 (58%) remained unchanged.
Conclusion: Oral fatty meal augmented HIDA scans may be helpful in selecting patients with ABS for surgery. However, surgeons should be cautious of a potentially high false-positive rate, leaving at least a third of patients with persistent pain after surgery.
Keywords: Acalculous biliary disease, Cholescintigraphy, Laparoscopic cholecystectomy
Introduction
Biliary symptoms are often described as a complex group of symptoms.
Some of the common complaints are gallbladder dyspepsia (episgastric
discomfort, flatulence, intermittent nausea with fat intolerance) and
biliary colic (abdominal pain localised in the right upper quadrant).
When biliary symptoms are associated with cholelithiasis, the treatment
of choice is usually cholecystectomy. However, patients with biliary
symptoms described earlier, but in the absence of gallstones on ultrasonography
(acalculous biliary symptoms, ABS) represent a complex group in whom
there may be multiple underlying causes for their symptoms. ABS can also
be mimicked by nonbiliary conditions such as the irritable bowel syndrome,
chronic hepatitis, gastro-oesophageal reflux disease, peritoneal adhesions,
irritable bowel syndrome, musculoskeletal or right-sided pulmonary disease.
Unlike patients who have gallstones and present with calculous cholecystitis,
patients with ABS often constitute a diagnostic and management challenge.
The main difficulty lies within selecting the group of patients who will
have good response to surgical treatment. The outcome of cholecystectomy
in patients without evidence of gallstones or acute cholecystitis is
variable. Sometimes, a proportion of patients continue to experience
abdominal pain postoperatively. Therefore, the decision to operate on
these patients should be carefully based on the clinical findings and
results of investigations such as cholescintigraphy.
Amongst patients
with ABS, there is evidence to suggest that a demonstrable abnormal gallbladder
ejection fraction (GBEF) of less than 35% can be predictive of
successful surgical outcome.[1] Technological
advances have enabled the outline of a gallbladder to be imaged using
intravenous radiolabelled agents like hepatic iminodiacetic acid (HIDA),
and the GBEF to be measured in response to a simultaneously administered
intravenous agent.[2] Conventionally,
intravenous cholecystokinin (CCK, or its active octapeptide, CCK-OP),
is used as a gallbladder stimulant in many centres. The efficacy of GBEF
derived from CCK-HIDA scan in predicting successful surgical outcome
has been reported in the literature to be high as 95%.[3] However,
there has been a decline of interest in using an intravenous gallbladder
as stimulating agents, and in many centres standardised oral fatty meals
are administered instead as a mean of stimulating gallbladder contraction
during HIDA scan. This change has partly been due to potential side effects
seen with intravenous agents. Furthermore, other stimulating agents such
as oral fatty meal is being increasingly recommended because of its more
physiological status [4] In
addition, oral fatty meals are easily handled by untrained department
staff, and are considerably less expensive. However, the use of fatty
meal has mainly been validated almost exclusively in healthy subjects [5],[6],[7] and
consequently, this practice has been criticised.[8]
The complexity of biliary dyskinesia or ABS combined with a growing familiarity
amongst surgeons in laparoscopic techniques therefore underscores the
need for diagnostic accuracy. In accordance to recent trends, our unit
changed from using intravenous CCK to oral fatty meal gallbladder augmentation.
Therefore, we wished to determine the clinical and histopathological
outcome of this group of patients with ABS who had undergone surgery
based on abnormal HIDA scans using a new radiological protocol (oral
fatty meal augmentation)
Materials and Methods
Patient selection for treatment and assessment
Patients who underwent HIDA scans between 1998 and 2001 were retrospectively
identified, and their case notes were reviewed. Relevant clinical details
were retrieved systematically using a predetermined proforma questionnaire.
HIDA scans were carried out in patients who have biliary symptoms such
as gallbladder dyspepsia (episgastric discomfort, flatulence, intermittent
nausea with fat intolerance), biliary colic (abdominal pain localised in
the right upper quadrant), but with no evidence of gallstone disease on
ultrasound scan. The decision to consider surgery was based on an abnormal
HIDA scan (GBEF of <35%), severity of symptoms, exclusion of nonbiliary factors that could mimic ABS, and patients′choice
with full counselling for risks of surgery involved. Patients who were
not fit for, or who decline surgery were used as controls. Cholecystectomies
were performed using standard laparoscopic techniques in all patients.
Postoperative clinical outcome was assessed as previously described by
others.[9] Each case was considered
a therapeutic ′success′ if preoperative symptoms resolved entirely or improved to such an extent that it no longer interfered with daily living. Inversely, if the patient had significant and persistent or new symptomatology and required further investigations, it was considered a therapeutic ′failure′.
Symptoms were judged according to the same criteria in the nonoperated
group.
All gallbladder specimens were examined using standard haemotoxylin
and eosin immunostaining techniques. They were grossly inspected for stone
content and wall thickness; sections were examined for hypertrophy, Rokitansky-Aschoff
sinuses, mononuclear infiltration, metaplasia, fibrosis, and other signs
of chronic inflammation. The presence of cholelithiasis excluded the related
patient from the study. Postoperative clinical success in the presence
of normal gallbladder histology was considered diagnostic of biliary dyskinesia.
Oral fatty meal augmented HIDA scan
Cholescintigraphy was performed following an over-night fast. One-hundred
MBq of 99 mTc-Mebrofenin [ N -(2, 4,
6-Trimethyl 3 Bromophenyl carbomoyl-methyl) iminodiacetic acid, that is,
Trimethyl-bromo-IDA or Hepatic IDA (HIDA) scan] was administered intravenously
(Cholecis ® Kit, CIS bio International, Schering Health Care Ltd., The Brow, Burgess Hill West Sussex, RH15 9NE). Imaging with a low-energy general purpose collimator positioned over the supine patient was commenced after 30 min. The acquisition time was 15 s per 128 x 128 element frame, and activity was recorded with a single-headed Elscint Apex SPX6HR gamma camera (Elscint Ltd., 13 Noah Mozes St., Tel Aviv 67442, Israel). A region of interest (ROI) was drawn around the gallbladder according to the distribution of activity. A similar ROI was drawn around an adjacent area of the liver to determine background counts. Scanning data was recorded in an Elscint Apex SPX1 NM Workstation. Corrections for radioactive decay were made by the workstation. At the time of peak gallbladder activity (as determined in a quantitative time-activity curve), or at most 60 min after the administration of radioisotopes, an oral fatty meal challenge was given (Kit-Kat ® chocolate
bar, 10.6 g fat content, total weight 48 g). Scanning continued for 25
min after ingestion. GBEF was calculated according to the formula GBEF
= [(Activitymax - Activitycontracted)/(Activitymax)], where 0.35 or more
was considered normal. No adverse clinical response to the fatty meal challenge
was recorded during scanning.
Results
Basic cohort data
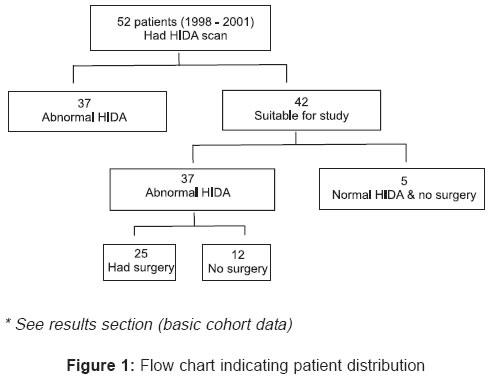
During the review period, 52 patients had HIDA scans for clinically
suspected chronic acalculous biliary disease. Four patients were lost to
follow up and six other patients were subsequently excluded due to a diagnosis
of cholelithiasis was made at surgery (prior ultrasound scans were negative
for gallstones). Forty-two patients were included in the study. The average
GBEF was 0.19 (range 0 - 0.59). Out of the 42 patients, 37 (88%) were found to have abnormal HIDA scan (GBEF < 0.35).
The average age was 43 years (range 20 - 68). One operation was converted
to an open procedure, and one emergency laparotomy was undertaken postoperatively
because of an intra-abdominal haemorrhage. About 5 of 42 patients had normal
HIDA scan and elected to have no surgery after being counselled for risk
of therapeutic failure [Figure - 1].
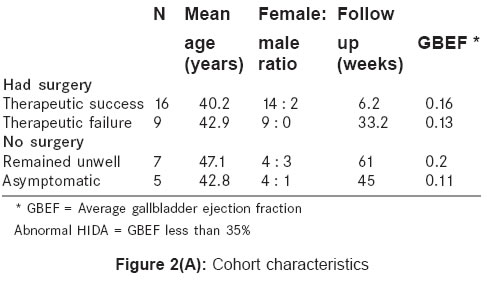
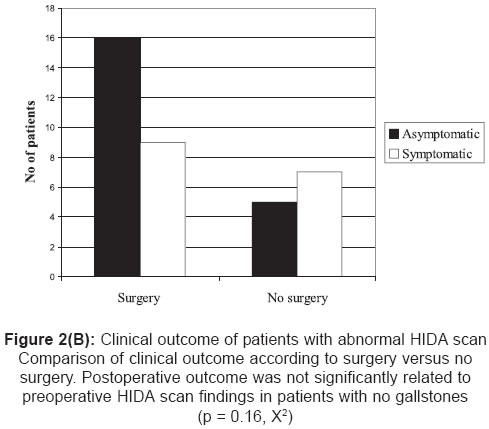
Analysis of clinical outcome
Amongst patients who had surgery, two-thirds of those operated [16
(64%), mean GBEF = 0.16] were noted to achieve therapeutic success. This group was followed up as outpatients for an average of 42 days. However, nine patients (36%, mean GBEF 0.13) failed to improve with surgery despite a mean postoperative follow up of 33 weeks. As for patients who did not undergo any operations, seven remained unwell (58%, mean GBEF 0.2) but five recovered spontaneously (42%, mean GBEF 0.11), after an average follow up of 45 weeks. Interestingly, out of five patients found to have normal HIDA and elected to have no surgery, 1 (20%) case was subsequently found to have peptic ulcer disease. The other 4 (80%)
cases became asymptomatic after a period of 12 months. No gastric or abdominal
pathology were found in these four patients [Figure - 2a] [Figure - 2b].
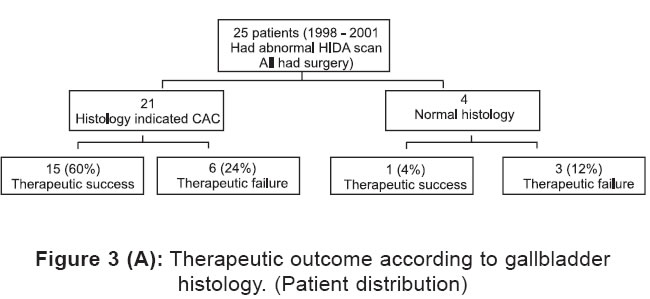
Histopathology
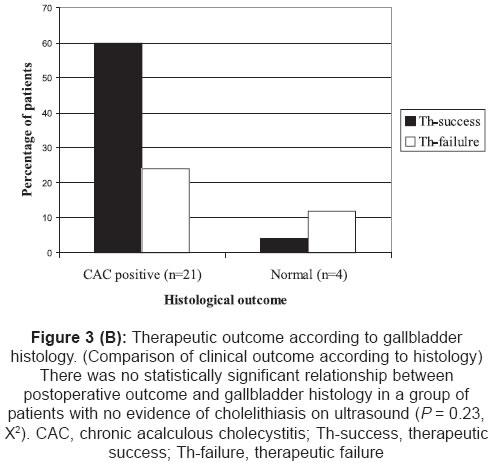
After surgery, 21 patients (mean GBEF 0.16) were found to have histopathological
evidence of chronic acalculous cholecystitis (CAC). Fifteen patients with
CAC (60%, mean GBEF 0.16) achieved therapeutic success. However, despite a mean follow up of 33 weeks, six failed to improve (24%, mean GBEF 0.14). Amongst four patients with normal gallbladder histology, 1 (4%) became asymptomatic and deemed cured (GBEF 0.12, biliary dyskinesia). However, three (12%) failed to improve after follow up of 25 weeks (mean GBEF 0.093). Out of nine cases, who did not achieve therapeutic success, six (67%)
of them has histological evidence of CAC [Figure - 3a] [Figure - 3b].
Discussion
Predictive value of oral fatty meal-HIDA scan
The present study also indicated that there is no statistically significant
relation between postoperative outcome and oral fatty meal-HIDA scan. Furthermore,
the therapeutic success rate is only just above 50%, which is relatively low. This low rate may have been owing to potential inherent methodological imaging flaw, causing inclusion of false positives. HIDA imaging is not without its criticisms. Gallbladder performance is known to depend on factors such as medication, hormones, and co-existing medical conditions, which must be taken into account when interpreting the HIDA scan. The choice of cut-off for GBEF (above which, indicates a normal gallbladder emptying) greatly influences the precision of the scan: a too high threshold giving rise to false positives, and a too-low threshold to false negatives. Chen et al. used 95% confidence
interval analyses to calculate the correct cut-off. Their local CCK-HIDA
scan protocol accepts a threshold of 0.28 to distinguish CAC from normal
gallbladders reliably.[10] Other authors have used other limits according to choice of intravenous triggering agents. Ziessman has even reported that the rate at which the CCK infusion is given will influence the cut-off: a doubled infusion rate raising the normal GBEF from 0.30 to 0.40 according to their protocol.[2] In the transition from intravenous to oral augmenting agents, the commonly used normal threshold of 0.35 has remained the standard. No studies have evaluated the sensitivity or specificity of oral fatty meal-HIDA scans in relation to subsequent surgery. The little research done has shown that there were significant differences in gallbladder response to different types of fatty meals.[11] Therefore, we simply do not know whether 0.35 is the correct threshold to use in the selection of candidates for cholecystectomy.
Another reason why cholecystectomy based on abnormal oral fatty meal-HIDA
scan has a low therapeutic success rate may have been because of the
range of biliary symptoms that patients have. For example, a group of
patients with right upper quadrant abdominal pain only may have a higher
therapeutic success rate than a group with epigastric bloating and dyspepsia.
Therefore, it would be interesting to perform subgroup analysis of therapeutic
success rate on different groups of patients, where each group has the
same presenting symptom. In other words, the new hypothesis is that oral
fatty meal-HIDA scan has higher predictive value in a subgroup of patients
who have perhaps less than one or two symptoms only. Unfortunately, due
to the small number of subjects in this study, subgroup analysis results
will not be meaningful and can be misleading.
Clinical outcome of nonsurgical therapy
In this study, despite evidence of abnormal gallbladder functions
based oral fatty meal-HIDA scan, patients who did not undergo surgery showed
a surprisingly high rate of spontaneous recovery (42%). This finding may have been due to the relatively small numbers involved. However, O′Neill and McCreath reported that 55% of
the nonoperated group was either subsequently attributed to other diagnoses
or resolved spontaneously.[12] Most
studies reported a high rate of success but failed to evaluate the outcome
of those (however small numbers they are) who remained symptomatic after
surgery. We felt that this small but significant group of postoperative
patients with ABS will require further evaluation so that the true benefit
of using HIDA imaging (either oral fatty meal or CCK augmented) to select
patients for surgery can fully be assessed.
Relation between postoperative outcome and histological finding
This study also indicated that 67% of operative failures (all
based on abnormal oral fatty meal-HIDA scans) were associated with histological
CAC. This finding seemed surprising because removal of histologically abnormal
gallbladders should be associated with cure. This paradox may have been
due to either insufficient follow up or small numbers. However, other authors
have reported similar finding, with mean follow-ups ranging up to 30 months.[10],[13] Interestingly,
by implementing a scheme for blind histopathological scoring, the number
of cases of CAC reported in this group of operated failures was reduced
by half.[14] This
suggests that histopathologists may have over-reported CAC and stricter
criterion for diagnosing the condition would be more appropriate. Conversely,
it may be possible that the prevalence of asymptomatic gallbladder inflammation
is higher than previously anticipated. In a study on the histopathology
of asymptomatic gallstones, Csendes et al. found that 33% of subjects
in the control group demonstrated mucosal pathology, most commonly CAC.
This finding was more common amongst older subjects.[15]
Length of postoperative follow up and ′cure rate′
Radiological criteria for the diagnosis of gallbladder disease largely
rest on the detection of calculi. However, in the absence of gallstones,
surgeons are often reluctant to carry out cholecystectomy in patients with
symptoms of gallbladder disease if the ultrasound scan is normal. Such
group of patients are often left with no satisfactory treatment. This study
showed that more than 60% of patients were recommended surgery, a figure that is in congruent with other published data. Unfortunately, a significant group of these patients are left with persistent abdominal pain. Evidence showed that long-period follow up may be required, if the full therapeutic effect of cholescystectomy is to be seen. We found that while a follow up of only 7 weeks was sufficient for cure to ensue in most of our patients, the remainder had derived no benefit from surgery after a mean follow up of 30 weeks. Although it is tempting to conclude that persistent symptoms after surgery will resolve in time, there is evidence that at least 5% will
remain so with 6 years follow up.[16] Conversely,
other authors have reported satisfactory outcomes with only minimal follow
up: Gunna et al. showed that abnormal fatty meal augmented HIDA scan is
predictive of at least 95% success rate with 10 months of follow
up.[17] Barron et al. used
CCK-OP augmented cholescintigraphy for patient selection, and achieve cure
in as many as 100% of patients on day 10 postoperatively.[18] No
suggestion has been made of how long it is acceptable for patients to wait
for cure to set in. If improvement is indeed due to gallbladder removal,
it seems reasonable to expect symptoms to resolve not long after the surgery.
Conclusions
0Management of patients with ABS is complex. We have not specifically compared
the efficacy of CCK-HIDA scans with oral fatty meal: HIDA scans. Only one
study compared the efficacy CCK injection with oral fatty meal during HIDA
scan. The results indicated that GBEFs created by oral fatty meal are significantly
lower, more variable, and ejection period is more prolonged.[7] The
change of radiological protocol for HIDA scan results in moderate benefits
only. However, we felt that oral fatty meal-HIDA scan in patients with
ABS has got a diagnostic role but it is conceivable that surgeons will
tend to over-rely on this investigation in selecting patients for surgery.
Although this study involved only a small number of patients, the failure
rate in operating on ABS patients based on oral fatty meal-HIDA imaging
is unacceptably high. In view of this, we cannot recommend surgery to ABS
patients with abnormal GBEF based solely on the usage of oral fatty meal
augmented HIDA scan.
References
| 1. | Patel NA, lamb JJ, Hogle NJ, Fowler DL. Therapeutic efficacy of laparoscopic cholecystectomy in the treatment of biliary dyskinesia: Am J Surg 2004;187:209-12. Back to cited text no. 1 [PUBMED] [FULLTEXT] |
| 2. | Ziessman HA. Cholecystokinin cholescintigraphy: clinical indications and proper methodology. Radiol Clin North Am 2001;39:997-1006. Back to cited text no. 2 [PUBMED] |
| 3. | Yap L, Wycheley AG, Morphett AD, Toouli J. Acalculous biliary pain: Cholecystectomy alleviates symptoms in patients with abnormal cholescintigraphy. Gastroenterology 1991;101:786-93. Back to cited text no. 3 |
| 4. | Balon HR, Fink-Bennett DM, Brill DR. Procedure guideline for hepatobiliary scintigraphy. Society of Nuclear Medicine. J Nucl Med 1997;38:1654-7. Back to cited text no. 4 |
| 5. | Fullarton GM, Meek AC, Gray HW, Bessent RG. Gallbladder emptying following cholecystokinin and fatty meal in normal subjects. Hepatogastroenterol 1990;37:45-8. Back to cited text no. 5 [PUBMED] |
| 6. | Hopman WPM, Rosenbusch G, Jansen JBMJ, de Jong AJL, Lamers CBHW. Gallbladder contraction: effects of fatty meals and cholecystokinin. Radiology 1985;157:37-9. Back to cited text no. 6 |
| 7. | Krishnamurthy GT, Brown PH. Comparison of fatty meal and intravenous cholecystokinin infusion for gallbladder ejection fraction. J Nucl Med 2002;43:1603-10. Back to cited text no. 7 [PUBMED] [FULLTEXT] |
| 8. | Middleton GW, Williams JH. Biliary scintigraphy in the investigation of acalculous gallbladder disease. (Letter) Nucl Med Comm 2001;22:602. Back to cited text no. 8 [PUBMED] [FULLTEXT] |
| 9. | Westlake PJ, Hershfield NB, Kelly JK, Kloiber R, Lui R, Sutherland LR, et al . Chronic right upper quadrant pain without gallstones: Does HIDA scan predict outcome after cholecystectomy? Am J Gastroenterol 1990;85:986-90. Back to cited text no. 9 |
| 10. | Chen PFM, Nimeri A, Pham QHT, Yuh J-N, Gusz JR, Chung RS. The clinical diagnosis of chronic acalculous cholecystitis. Surgery 2001;130:578-81. Back to cited text no. 10 |
| 11. | Kaplan GR, Charlesworth CH, Banarsee R. A Mars bar is not an adequate fatty meal - a comparison with Calogen. Clin Radiol 1995;50:180-1. Back to cited text no. 11 [PUBMED] |
| 12. | O'Neill GT, McCreath. An audit of biliary scintigraphyin a district general hospital (1993-1998) with special reference to the investigation of acalculous gallbladder disease. Nucl Med Commun 2000;21:829-34. Back to cited text no. 12 |
| 13. | Adams AB, Tarnasky PR, Hawes RH, Cunningham JT, Brooker C, Brothers TE, et al . Outcome after laparoscopic cholecystectomy for chronic acalculous cholecystitis. Am Surg 1998;64:1-5. Back to cited text no. 13 |
| 14. | Jones DB, Soper NJ, Brewer JD, Quasebarth MA, Swanson PE, Strasberg SM, et al . Chronic acalculous cholecystitis: Laparoscopic treatment. Surg Laparosc Endosc 1996;6:114-22. Back to cited text no. 14 |
| 15. | Csendes A, Smok G, Burdiles P, Diaz JC, Maluenda F, Korn O. Histological findings of gallbladder mucosa in 95 control subjects and 80 patients with asymptomatic gallstones. Dig Dis Sci 1998;43;931-4. Back to cited text no. 15 |
| 16. | Middleton GW, Williams JH. Diagnostic accuracy of 99Tcm-HIDA with cholecystoknin and gallbladder ejection fraction in acalculous gallbladder disease. Nucl Med Comm 2001;22:657-61. Back to cited text no. 16 |
| 17. | Gunna BR, Yannam GR, Kavita N, Pathak S, Alla BR, Acalculous biliary tract disorders: the value of fatty meal-cholescintigraphy, Surgeon 2003;1:293-5. Back to cited text no. 17 |
| 18. | Barron LG, Rubio PA. Importance of accurate preoperative diagnosis and role of advanced laparoscopic cholecystectomy in relieving chronic acalculous cholecystitis. J Laparosc Surg 1995;5:357-61. Back to cited text no. 18 |
Copyright 2005 - Indian Journal of Surgery
The following images related to this document are available:
Photo images
[is05059f3b.jpg]
[is05059f2a.jpg]
[is05059f2b.jpg]
[is05059f1.jpg]
[is05059f3a.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}