 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
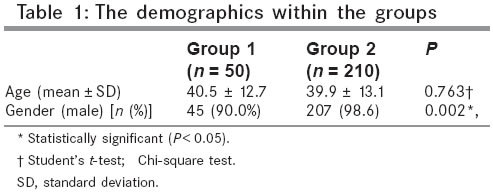
Indian Journal of Surgery, Vol. 67, No. 4, July-August, 2005, pp. 195-198 Original Article The effect of Ramadan fasting on duodenal ulcer perforation: a retrospective analysis Kucuk HF, Censur Z, Kurt N, Ozkan Z, Kement M, Kaptanoglu L, Oncel M Kartal Education and Research Hospital, 3rd Surgical Clinic, Istanbul, Turkey Code Number: is05060 Abstract Aims: The aim of this study is to evaluate the relation between Ramadan fasting and duodenal ulcer perforation, and to assess the risk factors for peptic disease in fasting Muslims.Settings and Design: Retrospective analysis was conducted for all patients, who underwent surgery especially in Ramadan for duodenal ulcer perforation in the emergency service between 1998 and 2003. Methods and Materials: Demographics, concomitant diseases, and predisposing factors were analyzed. Comparisons were done between patients, who were operated in Ramadans within a 5-year period (5 months during the study period) (Group 1) and on the remaining periods (55 months during the study period) (Group 2). Statistical analysis: Chi-square and Fischer's exact chi-square tests, Student's t-test and Mann-Whitney U-test were used. Results: Two hundred and sixty patients were included (50 in Group 1 and 210 in Group 2) in the study. The number of surgeries per month was statistically high in Group 1 than in Group 2 (10 patients per month vs 3.8 patients per month, P < 0.018). Predisposing factors play a major role and may be the reason for the difference. Conclusion: This study suggests that the incidence of duodenal ulcer perforation is relatively high in Ramadan among the people, who are fasting and have predisposing factors (especially history of dyspepsia). Therefore, we believe that people with predisposing factors and dyspeptic symptoms must be well informed and need special care. Keywords: Dyspepsia, Peptic ulcer perforation, Ramadan fasting Introduction Ramadan is the ninth month of the lunar calendar, during which it is obligatory for all healthy adult Muslims to fast during daytime. According to Islamic rules, those who cannot fast due to an illness or who have severe discomfort during fasting are exempted from Ramadan fasting. Although elective surgery has nearly vanished from the practice of general surgery owing to the improvement in the medical treatment of duodenal ulcer disease, the rate of emergency surgery for duodenal ulcers has remained stable in many areas since the 1970s.[1] Although, the relation between the pathogenesis of duodenal ulcer and Helicobacter pylori , nonsteroidal anti-inflammatory drugs, hyperacidity, and duodenal defense are well documented, there is insufficient data for the causative factors. The association between the time-restricted food and water intake, and the variations of gastric pH, plasma gastrin level has been known for a long time. [2],[3],[4] An epidemiological study has shown an increase in digestive disturbance during the first week of Ramadan.[5] Further, there has been a debate whether the patients with active duodenal ulcer can fast during Ramadan.[5],[6],[7],[8] Besides all these controversies, the relation between Ramadan fasting and duodenal ulcer perforations has never been evaluated in recent years. Therefore, the aim of this study is to evaluate the relation between Ramadan fasting and duodenal ulcer perforations and to assess the risk factors of this complication in Muslims who fast. Patients and methods This study is a retrospective analysis of patients, who received urgent operations for perforated peptic ulcer disease. A comparison was made between intensity of surgeries at Ramadan and all the remaining months of the year. This study was approved by the Kartal Education and Research Hospital Ethic Committee. A chart review was achieved for all the patients who underwent surgery for duodenal ulcer perforation in Kartal Education and Research Hospital Emergency Service between 1998 and 2003. Group 1 includes the patients, who were operated in Ramadan while fasting. Those who were operated during the remaining periods of the year were placed in Group 2. Demographics, concomitant diseases (e.g., diabetes mellitus, hypertension, chronic obstructive pulmonary disease), predisposing factors (e.g., history of dyspepsia, usage of nonsteroidal anti-inflammatory drugs, and presence of Helicobacter pylori ) were analyzed and data were compared within the groups. Multiple biopsies were taken from ulcer site during the surgery for Helicobacter pylori and ultrasound studies were done in early postoperative period to rule out hepatobiliary problems. History of smoking, chronic renal failure, liver disease, and hyperparathyroidism were evaluated. Statistics SPSS (Statistical Package for Social Sciences) for Windows 10.0 was applied for statistical analysis. The results were presented as percentages, or means and standard deviations. Categorical data were analyzed statistically with chi-square and Fischer′s exact chi-square tests and continuous data were analyzed with Student′s t -test and Mann-Whitney U -test. Results During the study period, 260 patients were operated for duodenal ulcer perforation in the emergency service. The median age was 40.0 ± 13.0 ranging from 20 to 85. Most of the patients were men ( n = 252; 96.9%). Fifty patients were operated for duodenal ulcer perforation in the emergency service during Ramadan (Group 1) and all these patients were regularly fasting at the time of Ramadan. Two hundred and ten patients were operated during the other periods of the year (Group 2). The demographics within the groups are depicted in [Table - 1]. There was no age difference between two groups ( P = 0.763), but men were significantly less in Group 1 (male patients in Group 1 were 45 (90%) vs 207 (98.5%) in Group 2, P = 0.002). The presence of concomitant diseases (e.g., diabetes mellitus, hypertension, chronic obstructive pulmonary disease) and predisposing factors (e.g., history of dyspepsia, use of nonsteroidal anti-inflammatory drugs, presence of Helicobacter pylori , smoking) within the groups are shown in [Table - 2]. Only three patients in Group 2 were diagnosed with gallbladder stone and there were no complaints of dyspepsia in these patients. There were no accompanying diseases such as renal and liver disturbances in both groups. Although, the presence of a concomitant disease (e.g., diabetes, hypertension, and pulmonary diseases) was significantly high in patients in Group 1 ( X2 = 4.81, P < 0.05), none of these diseases was separately significant within the groups (hypertension X2 = 2.19, P > 0.05; diabetes mellitus X2 = 2.59, P > 0.05; chronic obstructive pulmonary disease P = 0.479, >0.05). There was no statistical difference between the two groups in terms of smoking ( X2 = 0.08, P > 0.05). Presence of Helicobacter pylori did not show any difference between the two study groups ( X2= 0.82, P > 0.05). At least one predisposing factor was present in 46 (92%) patients in Group 1, and 179 (85.2%) patients in Group 2 ( P < 0.001). The number of the patients operated per month (per Ramadan in Group 1) was also calculated. There were 10 patients per Ramadan and 3.8 patients per month in Groups 1 and 2, respectively ( P < 0.018). The history for dyspepsia was the only predisposing factor that increased the risk of perforation in fasting people [38 (76.0%) in Group 1 vs 73 (34.8%) in Group 2, X2 = 28.09, P < 0.05]. Discussion The aim of this study is to evaluate the relation between Ramadan fasting and duodenal ulcer perforation and to assess the risk factors for peptic disease in Muslims who fast. In this study, men were dominant within the patients who underwent surgery for duodenal ulcer perforation. However, incidence of male dominancy significantly decreases in Ramadan (90.0 vs 98.6%, P = 0.002). Because there were only eight women in this study, it is not known whether it is an incidental finding, or whether women have a higher risk for duodenal ulcer perforation than men during Ramadan as Donderici et al. concluded in their retrospective study.[9] The concomitant diseases and predisposing factors were also calculated and compared within the groups. We found out that the number of the patients who had any of the studied concomitant diseases (e.g., hypertension, diabetes mellitus, or chronic obstructive pulmonary disease) were significantly high in Group 1 than Group 2. However, separate analysis revealed no statistical difference. Only three patients in Group 2 were diagnosed with gallbladder stone. There were no accompanying diseases such as renal and liver disturbances in both groups. This may be due to the limited number of patients in the groups, and further studies may reflect the relation between any of the diseases and duodenal ulcer perforation in Ramadan. It is impossible - with the data - to suggest any limitation of fasting in any of these patients. In this study, smoking did not play a role because there was no statistical difference between the two groups in terms of smoking ( X2 = 0.08, P > 0.05). Presence of Helicobacter pylori did not show any difference between the two study groups ( X2 = 0.82, P > 0.05), although it is very common in our country and is one of the predisposing factors for peptic ulcer disease. It has long been debate whether patients with active duodenal ulcer or at the risk of duodenal ulcer perforation may fast at Ramadan. Two separate studies from early 1950s showed the increased risk of duodenal ulcer perforation during the Ramadan.[10],[11] However, since then, many aspects have changed in duodenal ulcer management including anti-ulcer drugs such as histamine-2 blockers and proton pomp inhibitors or the availability of endoscopic examinations. A recent study has concluded that Ramadan fasting increases the risk of duodenal ulcer complications including hemorrhage and perforation.[9] In another study, Feldman et al. suggested that patients with acute duodenal or gastric ulcers should not fast, in order not to increase the risk of duodenal ulcer complications.[8] Similarly, Azizi claimed that patients with active duodenal ulcers should not fast, even when on treatment.[5] In contrast, in a recent study, endoscopic surveillance showed the cure of duodenal or gastric ulcers - including active bleeding ulcers - with an eradication therapy in 94.4% (17 of 18) in the fasting group and 95.5% (20 of 21) in the nonfasting group.[6] The authors claimed that Ramadan fasting is not risky even in patients with active ulcers. Similarly, in another prospective study with 57 patients, the investigators showed that patients with duodenal ulcer treated with lansoprazole might fast without running any risk.[12] During the study period, ten patients were operated per Ramadan and 3.8 patients per month during the other periods of the year ( P < 0.001) Thus, as previous studies have suggested - there is an elevated risk for duodenal ulcer perforation at the time of Ramadan. However, none of these studies have evaluated the risk of perforation in specific patients with predisposing factors or concomitant diseases. We have considered the history of dyspepsia and the use of nonsteroidal anti-inflammatory drugs as risk factors in this study, and we have observed that most of the patients, who were operated in Ramadan had any of these predisposing factors [84.0% (42 of 50) in Ramadan vs 56.2% (118 of 210) in the other periods of the year, P < 0.001]. Thus, the higher incidence of duodenal ulcer perforation at the time of Ramadan observed in this study is likely due to the higher number of patients, who had a predisposing factor, especially dyspepsia. The Ramadan fasting may be risky for the patients who have dyspepsia, and these patients should not fast. On the other hand, Ramadan fasting increases the risk for duodenal ulcer perforation in healthy population. Furthermore, Ramadan fasting increases duodenal ulcer or dyspeptic complaints. To conclude, this study demonstrated that incidence of duodenal ulcer perforation is relatively high in Ramadan among the people who are fasting. History of dyspepsia is an important predisposing factor for duodenal ulcer perforation in patients who are fasting. Patients with dyspepsia should be evaluated for peptic ulcer disease and if diagnosed should be treated before Ramadan fasting. However, those without any dyspeptic symptoms may fast during Ramadan. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05060t2.jpg] [is05060t1.jpg] |
| |||||||||

{kind=link}
{kind=link}