 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
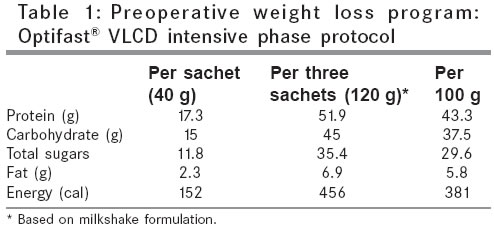
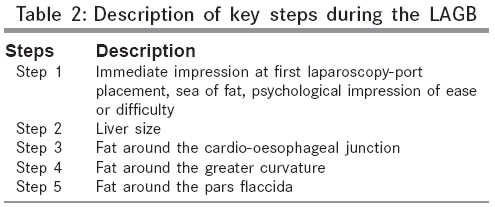
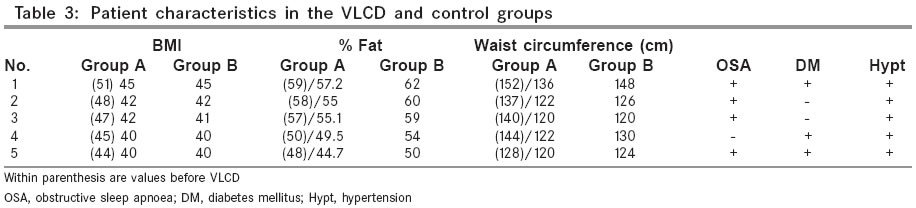
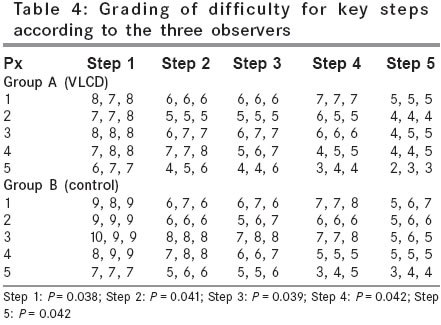
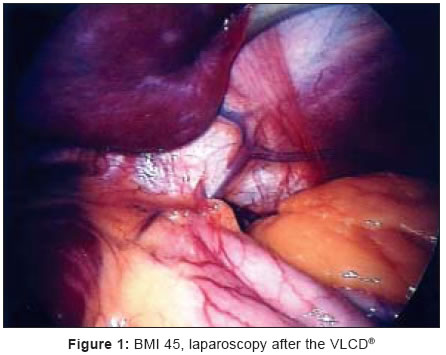
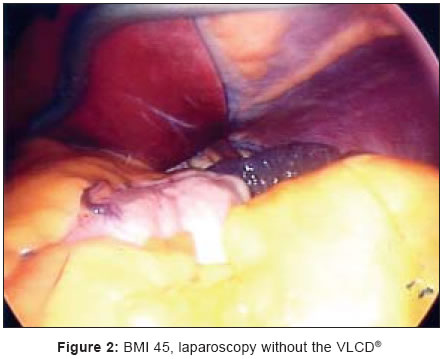
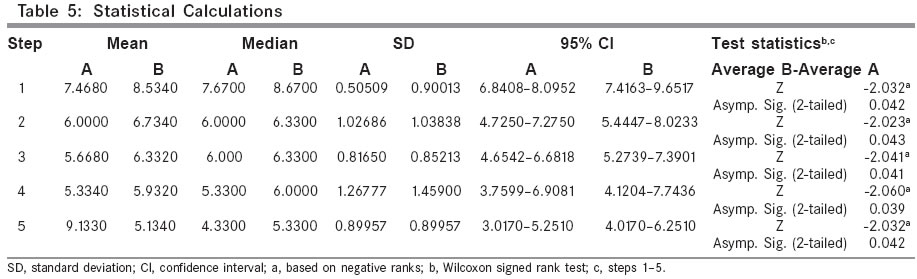
Indian Journal of Surgery, Vol. 67, No. 4, July-August, 2005, pp. 199-204 Original Article Laparoscopic adjustable gastric banding after the very low-calorie diet: Is it easier Rao A.D, Ganesh R, Baladas HG, Chan YH Department of Surgery, Weight Management Programme, Alexandra Hospital, Code Number: is05061 Abstract Background: Laparoscopic adjustable gastric banding (LAGB) is a bariatric surgical procedure that is worldwide accepted. However, it can be very difficult in super obese patients with body mass index (BMI) > 50. Much interest has been paid recently in performing the LAGB operation after an initial programmed weight loss with the use of the very low-calorie diet (VLCD).Aims: We sought to analyze the impact of the VLCD on the technical difficulties during the LAGB. Settings and Design: Randomized controlled trial. Materials and Methods: We evaluated prospectively, the technical difficulties for a single, dedicated bariatric surgeon during the LAGB in two groups of patients - patients operated on after 6 weeks on a VLCD diet (Group A, n = 5) and patients on no diet (Group B, n = 5). The two groups had similar BMI during the operation. The technical difficulties for five-key steps during the LAGB were graded by three individuals who were blinded with regard to the patient group. (1 = first surgeon, 2 = second surgeon, 3 = observer). Statistical methods: Cumulative values for each step and BMI level in the two groups were analyzed by the Wilcoxon signed rank test. Results: All three independent observers' grading of technical difficulties were found lower in Group A (P < 0.05) overall, as well as for each BMI value. Conclusion: Preoperative weight reduction with the VLCD made the LAGB technically easier in Group A. Keywords: Banding, Calorie, Diet, Difficulty, Gastric, Laparoscopic, Low, Obesity, Very Introduction 0The laparoscopic adjustable gastric banding (LAGB) is getting increasingly accepted owing to its safety, laparoscopy friendliness, acceptable weight loss, and absence of long-term adverse nutritional sequelae. Like all other laparoscopic procedures extreme operative difficulty is encountered in the super obese patients (BMI > 50). Of late, many have resorted to preoperative very low-calorie diet (VLCD) for a fixed period of time followed immediately by the LAGB. This is unlikely to reduce operative risk significantly, though what seems logical from the surgeon′s point of view is that a preprogrammed weight reduction immediately before operation is likely to make the operation technically easier, which subsequently translates into a lowered operative risk and lowered morbidity. From our empirical experience with bariatric practice in general, we are inclined to believe that diet restriction-related weight loss first affects the viscera, and if this is carried out scientifically with a calculated very low-caloric intake under supervision, one can achieve significant reduction in visceral fat volume which we believe translates into easier laparoscopy. Circumference measurements in the trunk area are known to show significant short-term changes in response to fasting, which probably can be explained by a preferential fat reduction from the visceral region as compared to other body fat depots. In the Asian setting, the experience with super obese patients is limited, unlike in the Western world. However, BMI for BMI, the Asian patient is likely to qualify as super obese at much lower values. Most of the experience with VLCD is from the Western world and many authors have commented about the procedure becoming slightly easier after the VLCD. The principal reason for this is likely to be the reduction in visceral fat predominantly after rapid early weight loss, which makes laparoscopy easier. This is of interest in the Asian setting because according to the author who has an experience of more than 150 cases in the Asian population, LAGB is more technically challenging in the Asian patient than his Caucasian counterpart for the same BMI values owing to differences in frame and body build. This makes it all the more necessary to evaluate the role of preoperative VLCD in the Asian setting and set guidelines for its use as the observed difference is likely to be more significant in the smaller Asian patient.Materials and methods We allocated patients (eight men and two women) into two groups. Group A (study group, n = 5) consisted of patients who came to surgery after 6 weeks of VLCD-induced weight loss (OPTIFASTÒ VLCD - Novartis Medical Nutrition, 445 State Street, Fremont, MI 49412, USA). Group B (control group, n = 5) consisted of patients with extremely high BMI who were subjected to LAGB without preoperative VLCD. The two groups had similar BMI at operation. Ten eligible patients during the period August-September 2004, with requisite BMI values were chosen randomly by a neutral nurse in the weight management clinic. Attempts were also made to match the patients in either group as far as possible in other physical parameters like sex, height, weight, percent fat, age, and comorbidities apart from the stated BMI criteria. The VLCD protocol involved a period of supervised intake of the prescribed diet after ward admission for 3 days followed by weekly follow up. The investigations during ward admission included daily electrolytes, urea levels, ECG, and urine ketones. Blood glucose was monitored three times daily during admission. The VLCD was provided to patients in packets in the form of powder mixed with cold water in a choice of three flavors; chocolate, vanilla, and strawberry. The study protocol required the patients to consume three shakes per day (456 Cal) [Table - 1]. The VLCD was administered for a total period of 6 weeks followed by repeat measurements of BMI and other variables. The VLCD administered patients were only allowed two additional oil-free salad helpings per day in addition to the VLCD. The full period of VLCD admission was closely supervised by a physician in addition to the surgical team. The tests were based on the guidelines set by Novartis Nutrition (Preoperative Weight Loss Protocol, www.novartis.com.au) and included daily electrocardiogram apart from daily urinary ketones, blood glucose, and electrolytes every alternate day. The selected patients were randomized by a neutral researcher from the weight management clinic after ethical clearance from our institutional review board and informed consent from each patient. All three graders were blinded to the VLCD status of the patients and the patients came to the surgery in random order with triplicate grading forms in sealed envelopes. Our bariatric surgical division is run as a part of an overall weight management program. Patients with high BMI, undergo a 6-month period of diet counseling and exercise regimen. Patients are referred for surgery after a reasonable period of failed attempts of nonsurgical methods of weight loss. Workup consists of routine tests to assess fitness for anesthesia including urinary-free cortisol levels and a routine polysomnogram to detect obstructive sleep apnoea. We performed the LAGB using the pars flaccida technique. All patients in this study were banded using the BioEntericsÒ LAP-BANDÒ system (INAMED, 1035 CINDY LANE CARPINTERIA, CA 93013, USA). The key steps in the LAGB procedure that would affect the difficulty of performing the operation and subsequently the main outcome parameters are given in [Table - 2] and they would be influenced favorably by loss of visceral fat. The three graders (observer 1 - first surgeon, observer 2 - second surgeon, observer 3 - observer from the weight management team) graded each LAGB procedure independently on the basis of the degree of difficulty on a scale of one to ten (1 denotes - least difficult, 10 denotes - most difficult). Three observers graded each identified step independently. The results were analyzed for each key step and as a cumulative value for each patient (i.e., for each BMI value in either group). The operator grading were analyzed using the Wilcoxon signed rank test. The main end point of the study was the summated value for each step and cumulative value for each BMI level, which were compared in both groups[Figure - 3]. Results The patient characteristics in the VLCD patients (Group A) and control patients (Group B) are given in [Table - 3] and the grading of the key steps is shown in [Table - 4]. Eight males and two females were included in the study. The two females belonged to the BMI Group 3. The values in the tables show the fat percent to be slightly higher in the non-VLCD patients for their matching BMI counterparts. The same trend is reflected in their waist circumference values. However, whether this trend is statistically significant remains to be established with studies enrolling higher numbers. The figures show the differences at first appearance at laparoscopy between the post-VLCD and non-VLCD patients [Figure - 1] and [Figure - 2]. The figures aim to depict the obvious difference in degree of difficulty encountered at first impression on laparoscopy. The descriptive statistics for each group are shown in the [Table - 5]. We had no mortality and all patients in this study were discharged on the first postoperative day after a normal upper gastrointestinal contrast study (ultravist swallow) and requisite dietary advice. The operator grading was analyzed using the Wilcoxon signed rank test and significance was set at P < 0.05. The test statistics and z values for the tests are shown in the corresponding calculations. All three independent observers gradings of technical difficulties were found lower in Group A ( P < 0.05) overall, as well as for each BMI value. Discussion The LABG is an efficient and safe operation.[1],[2] Studies have shown that fat mass and lean body mass decrease significantly more in VLCD-treated subjects than in other forms of diet control.[3] The mechanism of the enhanced weight loss in the group with very low-carbohydrate diet is not clear.[4] There have been reports of visceral fat being mobilized faster than subcutaneous fat in experimental studies. This probably translates into a more than externally visible outcome from the point of view of subsequent laparoscopic surgery as the authors of this paper endeavor to prove. The senior author of this paper, who has the largest experience of LAGB in Asia, with about 200 cases to date, has many dedicated bariatric surgeons the world over concurring with him. According to him, a preprogrammed short duration of VLCD-induced rapid weight loss can be safely achieved in the outpatient setting after an initial short period of observation. The difficulty in grading for each step show that the post-VLCD patients form an easier operative group at each analyzed step of the operation. Overall, Group A also seems to be an easier group from the point of view of all the graders. According to some reports, best predictors of body density in obese women before and after weight loss are circumference measurements in the trunk area.[5] Many literature reports say that waist circumference may not offer additional information about abdominal fat distribution. [6],[7],[8],[9],[10] To date, BMI is probably the only single, objective factor to decide the extent of extremeness of intra-abdominal obesity. In our study, the post-VLCD-lowered BMI of patients in Group A matched with the BMI in Group B. In a study by Pare and associates, to examine the association of waist girth changes in predominantly abdominally obese men after short-term weight loss, there was a greater relative reduction in visceral adipose tissue volume against the subcutaneous adipose tissue volume.[11] Our interpretation of pilot studies in obese patients undergoing the LapBand surgery is that visceral fat is mobilized faster than the other fat deposits. This finding is supported by literature reports of studies analyzing gene expressions in visceral and subcutaneous fat in response to fasting. [12],[13],[14],[15] Adipose tissue located within the abdominal cavity has been suggested to be functionally and metabolically distinct from that of the subcutaneous compartment and intra-abdominal fat is also independently associated with liver fat, whereas subcutaneous fat is not.[16] In response to dieting, the greatest change occurs in the preperitoneal fat layer. This is why, there is only a slight decrease in WHR (waist-hip ratio) after the VLCD and hence, the WHR is not useful in quantifying intra-abdominal fat loss. [17],[18],[19],[20] Subjects with large initial amounts of intra-abdominal, preperitoneal, and visceral fat have been shown to lose more fat during weight loss.[21] Sonography seems to be useful in monitoring small variations in the thicknesses of subcutaneous abdominal and intra-abdominal preperitoneal and visceral fat.[22] As an index of intra-abdominal fat accumulation, the ratio of the intra-abdominal visceral fat area to subcutaneous fat area, determined by a computerized tomographic section at the level of the umbilicus can be used in future studies for quantitative assessment of fat reduction.[23] Waist-hip ratio (WHR) and abdominal sagittal diameter (SagD) are generally measured as indicators of fat distribution, and visceral adipose tissue (visceral AT) can be estimated by anthropometric computerized tomography calibrated equations.[23] Total visceral fat measurement is said to accurately identify small intra-abdominal fat variations. In most published studies, WHR could not evaluate visceral fat loss, because of simultaneous decreases in waist and hip circumferences. Hepatic fatty infiltration is also not always uniform. According to Toouley et al. there is a significant decline in liver size after a 6-week VLCD therapy, thereby making upper GI laparoscopic procedures easier. Two sequential CT scan examinations, performed before and after diet therapy, may be useful for evaluating obese patients with elevated serum transaminase and predicting ease of lapBand.[24] According to some studies, abdominal height is a powerful, independent predictor of ALT in both sexes, as well as of GGT among women in cases with morbid obesity, and these findings support a role for central adiposity independent from BMI in predicting increased levels of hepatic enzymes, likely as a result of unrecognized fatty liver.[25] Hepatomegaly was associated with visceral obesity in morbidly obese women with liver steatosis. The phase of rapid weight loss after gastric surgery is associated with a significant reduction in liver volume.[26] Where absolute and relative reductions in body weight and body fat are similar, men mobilize more intra-abdominal fat than women, whereas women lose more subcutaneous fat. The greater reduction in intra-abdominal fat seen in men is accompanied by a more pronounced improvement in the metabolic risk profile. Therefore, greater improvement of risk factors in men is not only related to a greater negative energy balance, as shown in most studies, but is also sex-specific.[27] In spite of our very low-sample size, an overall statistical analysis comparing the two groups is possible, particularly taking into account a marked homogeneity of estimated difficulties by three independent graders. It must however be noted that such a small sample size probably lends itself to a Type I statistical error. Future studies should be directed towards objective measurements of fat content in different visceral compartments and the amount of volume reduction after caloric restriction. Initial experience, albeit with our small number of cases has shown that the VLCD is a very good primer to make laparoscopy easier for the bariatric surgeon, particularly in the super obese. It probably does have a psychological component to it. With our initial experience, we also firmly believe that such studies are better performed when the surgeon is ideally on his learning curve.References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05061t1.jpg] [is05061t4.jpg] [is05061t3.jpg] [is05061t2.jpg] [is05061fl.jpg] [is05061f1.jpg] [is05061t5.jpg] [is05061f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}