 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
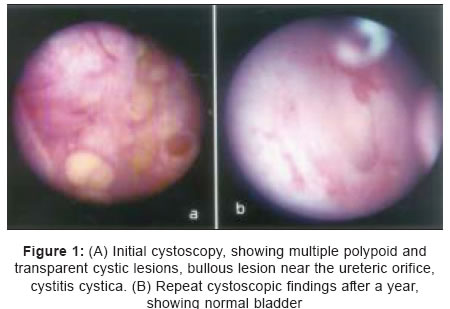
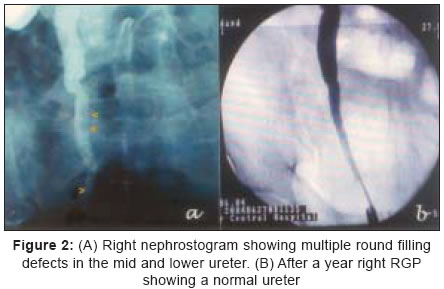
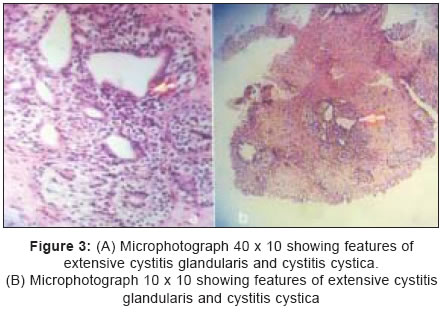
Indian Journal of Surgery, Vol. 67, No. 4, July-August, 2005, pp. 210-212 Case Reports An unusual case of obstructive uropathy: Cystitis cystica with ureteritis cystica Zaharani, AhmedBakheet, Soundra Pandyan GV Department of Urology, Assir Central Hospital, Affiliated to King Khalid College of Medical Sciences, Abha Code Number: is05064 Abstract A 45-year-old man presented with loin pain and burning micturation. He had a positive Bilharzial titre and impaired renal function. Ultrasonography (USG) revealed right hydroureteronephrosis and a thickened bladder wall with areas of calcification. A diuretic 99mTc - DTPA scan (technetium-99m diethylene triamine penta acetic acid) showed features of obstruction in both the kidneys. Cystoscopy showed polypoid transparent cystic lesions obscuring both the ureters. The obstruction was relived by percutaneous nephrostomy (PCN). Nephrostogram showed multiple scalloped filling defects in the right ureter with obstruction at the uretero vesical junction (UVJ), suspicious of ureteritis cystica (UC). Biopsy of the lesions showed features of Bilharzial proliferative cystitis with extensive cystitis glandularis and cystitis cystica (CC). Complete cure was achieved by semi-interventional methods and prompt treatment of the underlying infection. Diagnosis, management, and progression of this case with review of literature are discussed.Keywords: Cystitis cystica, Obstructive uropathy, Ureteritis cystica Introduction 0Cystitis cystica (CC) and ureteritis cystica (UC) are uncommon benign proliferative lesions of the urothelium. Formation of submucosal cysts under the urothelium, appear as filling defects in urogram confusing the diagnosis. This patient presented with loin pain only and a past history of Bilharziasis. A diagnosis of obstructive uropathy with renal failure was made initially. Only after cystoscopy, biopsy, and nephrostogram a diagnosis of CC with UC was possible. Conservative treatment of the E. coli and Bilharzial infection, with relief of the associated obstruction with semi-interventional methods and regular follow resulted in complete regression of the lesions. Association of CC and UC together in the same patient, presenting primarily as obstructive uropathy and complete regression after treatment of underlying cause is noteworthy in this case.Case report A 45-year-old male Egyptian farmer presented with history of, severe right loin pain and burning micturation since 2 weeks. There was history of urinary Bilharziasis since childhood. On examination, he looked ill with pain and his right kidney was palpable and tender. Results of routine investigations were normal. He had a raised Bilharzial titre-1 : 2560 and creatinine level of 3.2 mg. Urine culture grew E. coli. Ultrasonography (USG) showed severe right hydroureteronephrosis. Left kidney also had mild hydronephrosis. The urinary bladder was thick walled with areas of calcification. Plain CT scan of the KUB area confirmed the USG findings. A course of Praziquantel was given and the E. coli infection was treated. A rising serum creatinine level (5.2 mg) and persisting loin pain warranted an immediate intervention. Cystoscopy showed multiple polypoid, and transparent cystic lesions of different sizes [Figure - 1]A in the bladder. It was impossible to visualize the ureteric orifices. Multiple biopsies were taken from the lesions and bladder wall. The obstruction was drained by a right percutaneous nephrostomy (PCN). Right nephrostogram showed multiple scalloped areas with semi-circular filling defects [Figure - 2]A in the middle and lower ureter with obstruction at the Uretero Vesical Junction (UVJ). Obstructive uropathy secondary to UC and CC was provisionally diagnosed. The patient′s pain and creatinine value improved postoperatively. Histopathology showed features of Bilharzial proliferative cystitis with extensive cystitis glandularis and CC [Figure - 3]A & B. There was no evidence of malignancy. Ultrasonography repeated after a month showed reduced hydronephrosis of the right kidney. A diuretic 99mTc - diethylene triamine penta acetic acid (DTPA) scan showed features of obstruction in both the kidneys with more delay, in diuretic wash out on the left side (right kidney 36%, left kidney 64%). Repeat cystoscopy showed marked regression of the lesions. The left ureteric orifice could be seen. But the right ureteric orifice was still masked by the lesions. Because attempted retrograde stenting of the left kidney failed a left PCN was done. Left nephrostogram showed dilated left ureter till the UVJ with partial obstruction but with no features of UC. Following another month, there was further improvement in renal impairment and the CC lesions. Percutaneous nephrostomy′s were removed and retrograde stenting on the right side with antegrade stenting on the left side was done. Three monthly follow up with repeat cystoscopy and change of stents was done for a year. After a year the stents were removed without reinsertion. The renal functions returned to normal and the bladder and ureter no more showed features of CC or UC [Figure - 1]B. Two years later repeat cystoscopy showed no further recurrence [Figure - 2]B.Discussion Cystitis cystica and ureteritis cystica are uncommon clinical entities that one comes across in urological practice. Reported first by Morgagni, it was described in detail by Richmond and Robb.[1] It is often seen in older patients and uncommonly in pediatric group. The etiology, morphology, and clinical significance of these lesions are poorly understood. It commonly involves the bladder neck and trigone area and occasionally the ureters and pelvis. Causative factors such as infection, irritation, and inflammation to carcinogens have been incriminated. Initially considered to be a premalignant disease of the urinary bladder, it is now considered as an association with malignancy. It reflects mobilization of the humoral immune defense mechanism in response to various agents, among these to a subclinical malignant tumour.[2] There are case reports of association of UC with adenocarcinoma of ureter[1] and more recently CC with adenocarcinoma of bladder and pelvic lipomatosis.[3] Jost et al. describe the ultra structural features of CC observing, that the wall of each cyst consisted of a 2-3 layered epithelium with either tall columnar or flattened cells and with short microvilli. The columnar type also contained numerous membrane-bound, electron dense secretory granules in the apical cytoplasm.[4] A wide variation in staining for MIB-1, p53, p27 and cytokeratin 20 in both florid von Brunn nests and nested variant of urothelial carcinoma was noted by Volmar et al. They could not get a specific cutoff value for diagnostic purposes. They stressed the importance of morphologic assessment in the distinction of these two entities.[5] Apart from pain and features of urinary infection, there is no specific symptom in CC or UC with which the patient can present to help in suspecting the condition. Contrast imaging studies shows typical smooth filling defects in the wall of the urothelium. While it can help in suspecting the condition there are other commoner conditions to consider in the differential diagnosis (radiolucent calculi, polyps, papillary tumours, blood clots, uro-tuberculosis, air bubbles, and infections due to gas forming organisms). The gold standard in the diagnosis of CC and UC is still by cystoscopy, retrograde pyelogram, ureteroscopy, and biopsy of the lesion. A plethora of treatments ranging from simple observation, treatment of infection, removal of irritant, excision of the lesion, TUR[6] to more extensive procedures such as resection of bladder, ureter, and PUJ have been reported. Silver nitrate, chlorhexidene bladder installation have been used successfully. Neodymium-YAG laser has been used successfully to treat a resistant case.[7] Aabech and Lein reported CC in 97/437 girls during cystoscopy done for recurrent urinary infection. They have suggested long-term treatment with follow up.[8] Progression of CC and UC to carcinoma is rare. Long-term follow up studies of cases for 17 years[9] and in another study for 6.5 years have shown no evidence of carcinoma. However, patients with extensive metaplasia are to be followed up regularly. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05064f3.jpg] [is05064f1.jpg] [is05064f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}