 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
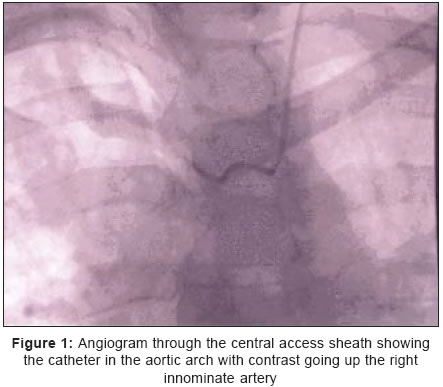
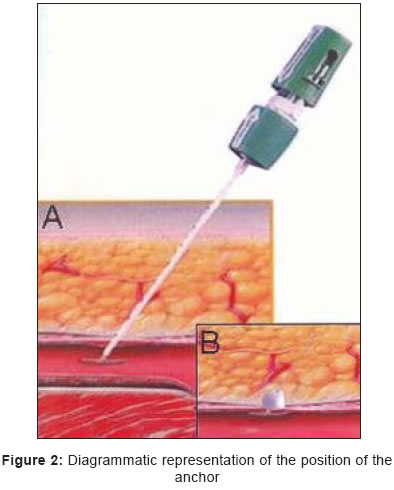
Indian Journal of Surgery, Vol. 67, No. 4, July-August, 2005, pp. 213-215 Case Reports A simple method of closing an iatrogenic subclavian arterial puncture Abbas M, Hamilton M, Yayha M, Angel D, Mwipatayi BP, Sieunarine K Department of Vascular Surgery, Royal Perth Hospital, Perth, WA, Code Number: is05065 Abstract Central venous catheters are the mainstay in the intensive management of surgical patients today and they have increasingly been applied in different medical specialties and for different clinical indications. It is generally safe to place central venous catheters using anatomic landmarks alone, but there are some possible immediate, early, and late complications related to the implantation technique. One particularly dangerous vascular complication is inadvertent arterial sheath placement. When this occurs in a site that is anatomically non-compressible, sheath removal can necessitate surgery or exposure to a significant risk of haemorrhage with manual pressure. We report a case of a sheath that was inadvertently placed in the subclavian artery and was successfully removed using a percutaneous vascular closure device.Keywords: Central venous access, Subclavian artery, Percutaneous closure device Central venous access is the preferred method of access for patients undergoing surgical procedures, during resuscitation and fluid management in intensive care. Many reports have been published about the complications associated with it. Central venous access is routinely done using the internal jugular vein or the subclavian vein. In both approaches there is a risk of inadvertent puncture of the corresponding arteries. The consequences of subclavian arterial puncture are not as potentially serious as the consequences of inadvertent internal carotid puncture during attempted internal jugular venepuncture, which potentially include a cerebral thromboembolic event or airway compromise from bleeding. However, bleeding from the subclavian artery is much more difficult to control by pressure alone due to limited access because of the clavicle. Also, bleeding may be easily missed because the blood may track into the pleural cavity. Because of these reasons the subclavian route is generally thought to be the least suitable approach to the central circulation in the anticoagulated patient. We report a case of immediate simple closure of the puncture site in a subclavian artery with Angio-Seal (St. Jude Medical), a percutaneous vascular closure device. CASE REPORT A 54-year-old male with a history of infected left shoulder injury was admitted and underwent surgical debridement of the shoulder wound and intravenous antibiotics. Following debridement of the wound a central venous access was placed for intravenous antibiotics. After placement of the central venous catheter when the intravenous fluid bag was connected, due to difference in pressures blood was noted to be reversing back into the intravenous fluid bag. The intravenous access was clamped immediately and the vascular surgeon was notified. The patient was taken for angiography. Angiography via the catheter revealed contrast flow in the right innominate artery [Figure - 1] due to arterial position of the catheter. To reduce the potential for bleeding it was decided to remove the catheter and close the puncture site with a percutaneous vascular closure device (Angio-Seal, St. Jude Medical). A 0.035" guide-wire was placed through the misplaced central access catheter and the catheter was slowly withdrawn to lie in the arch of aorta, so that the guide-wire could be stabilised before removing the catheter. The existing central catheter was removed and the Angio-seal STS Platform sheath dilator assembly was advanced over the guide-wire. The assembly was manoeuvred to confirm proper position of the sheath tip within the artery. The dilator and guide-wire were then removed and the Platform device and sheath were locked together. The anchor was pulled against the sheath tip which was then positioned at the inner arterial wall puncture site [Figure - 2]. Slight tension was then applied to the suture as it was cut below the skin level. The patient tolerated the procedure well and was shifted back to the ward for further management of his shoulder wound. There were normal pulses at the wrist region after the procedure and on discharge. The patient was discharged from the hospital with no untoward complication after 3 days.DISSCUSSION Inadvertent arterial puncture during the placement of the central venous catheter is a well known complication and has been reported to be up to 3.7%.[1] Also, it has been reported that the complication rate has been directly proportional to the number of attempts made, and some have recommended that more than 3 attempts can give a complication in nearly 1 case over 2.[2] Inadvertent subclavian arterial puncture is one of the commonest complications with subclavian venous access even though it is not as serious a complication as an inadvertent carotid puncture which may potentially lead to stroke and disability. When access catheters are inadvertently placed in the subclavian artery, the risks may involve arterial occlusion, embolism, pseudoaneurysm, dissection,[3], [4] and fatal exsanguinations.[5] Although misplaced venous catheters may be removed with direct compression, some arterial sites such as the subclavian artery are non-compressible because of their anatomic location. Other risk factors contributing to complications include obesity, previous surgery or radiotherapy of the area, previous central venous catheters, multiple needle passes and inexperience.[1] Removing the catheter with a wait-and-see strategy is no longer recommended these days with documented complications as mentioned before and also with the availability of minimal invasive techniques. Several options have been reported in the literature in the management of the inadvertent subclavian arterial puncture. Surgical repair usually requires partial removal of the first rib or thoracotomy. However, patients requiring central venous catheterisation are usually very ill and thoracotomy has high morbidity and mortality. The next option is percutaneous stent-grafting of iatrogenic arterial bleeding and pseudoaneurysm, which is recognized as a successful treatment with a low complication rate compared with surgery.[6] Percutaneous stent-grafting can be the preferred approach in subclavian artery injury rather than in just an inadvertent puncture, where less expensive devices can be used. Intra-arterial balloon compression for subclavian artery puncture during central venous catheter introduction or pacemaker lead placement has been reported.[7] Local percutaneous treatment [8] has recently been reported for inadvertent arterial punctures. Several case reports have documented the complications associated with arterial closure devices[9] but they are generally safe with reduced morbidity over other procedures. The Angio-Seal device (St. Jude Medical) used here relies on a small collagen plug on the outside of the artery, held against the arteriotomy site by a small collagen footplate inside the artery. It is recommended for use after up to 8 Fr catheter insertion. For larger arteriotomies the percutaneous suture device has been recommended. In summary, inadvertent subclavian arterial puncture can be successfully managed using a percutaneous vascular closure device with no adverse clinical sequelae. The technique is relatively straightforward, especially for those who are familiar with the device. It may be an option for patients with non-compressible arterial punctures who are not good surgical candidates provided the puncture site is less than 8 French in size. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05065f2.jpg] [is05065f1.jpg] |
| |||||||||

{kind=link}
{kind=link}