 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
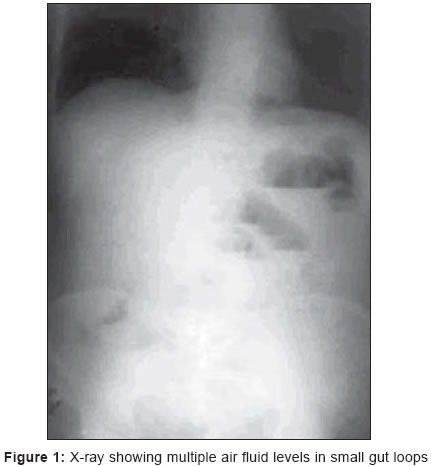
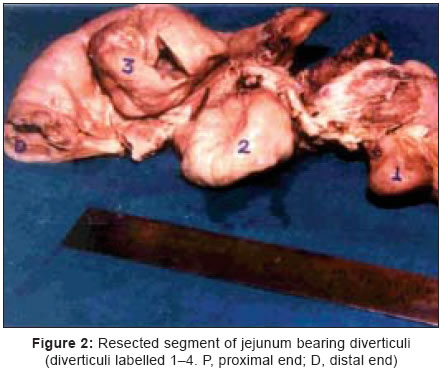
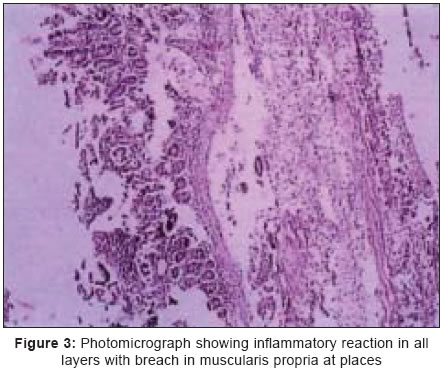
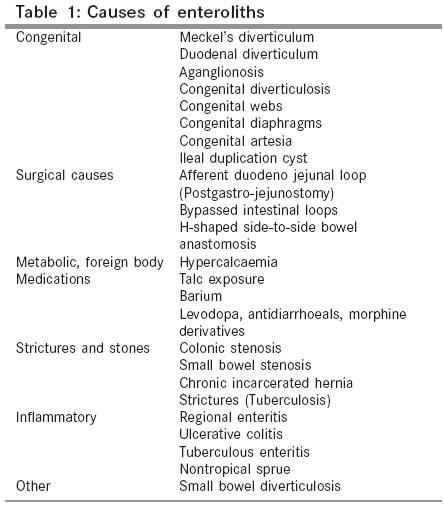
Indian Journal of Surgery, Vol. 67, No. 4, July-August, 2005, pp. 219-221 Case Reports Jejunal diverticulosis with enterolith - presenting as acute intestinal obstruction Batra RajenderKumar, Sandhu NS Consultant Surgeon, Kaiser Hospital, Sector - 21, Panchkula, Haryana, Code Number: is05067 Abstract The case of a 55-year male, who had acute small intestinal obstruction due to jejunal diverticuli and a large (5 x 4 cm) stone (enterolith) is presented here. The stone however could not be detected before surgery on plain X-ray abdomen. The patient was resuscitated and within a few hours taken up for surgery. Barring an inflammatory band from jejunum till sigmoid colon, rest of the colon was normal. Resection of jejunal segment bearing four large diverticuli was performed and stone was removed from distal end of resection. Although, diverticulosis is rare and an unsuspected cause of acute small intestinal obstruction, it occurs in about 1-7% of cases. This case being an emergency, the investigations were limited and the diagnosis and treatment plan was to be decided at laparotomy Keywords: Acute intestinal obstruction, Diverticulosis, Enteroliths Introduction Acute small intestinal obstructions are mostly due to adhesions after earlier surgery or hernias or to some extent malignant neoplasm. In cases where intermittent small intestinal obstructions occurs and no prior abdominal surgery is performed, the causes under consideration are multiple jejunal diverticulae with enteroliths, which may extrude and produce mechanical obstruction. In World literature that is available on Medline and Pub Med on the relevant topic, reports only 34 cases that have duodenal or jejunal diverticuli with enteroliths presenting with small intestinal obstruction. The interesting feature is its varied clinical presentation and limited exposure to surgeon in making correct preoperative diagnosis. The presentations vary from uncomplicated recurrent obstruction to complications such as signs of bowel ischemia, perforation or malena.[1],[2] The CT scan, MRI or Barium studies could only be performed in cases with sub acute or recurrent intestinal obstruction. Hence, from the literature review available, a definite guideline can be prepared as to how these cases can be managed without leaving it on personal surgical experience and choices. CASE Report A 55-year-old man with no previous abdominal surgery, a smoker and alcoholic for the past 15 years presented in emergency department with acute abdominal pain, constipation, and abdominal distension of 3-day duration. He had h/o malena 10 days before this episode. Abdomen was distended, soft with localized guarding and tenderness in left lumbar and umbilical region. X-ray abdomen showed multiple air fluid levels in small gut loops, with dilated cecum, ascending and transverse colon [Figure - 1]. The clinical diagnosis of acute intestinal obstruction due to suspected growth in descending colon was made and the patient was taken up for exploratory laparotomy within 3-4 h of admission, and so no other investigation was performed. On laparotomy, it was found that there was seropurulent fluid about 500 ml, multiple adhesions of omentum with colon and jejunal diverticulae which were four in number on the lateral wall of jejunum starting one foot from duodeno-jejunal junction to about 2 ft of jejunal loop [Figure - 2]. There was a 5 x 4 cm size fecolith in distal jejunal loop causing obstruction, and an adhesion of sigmoid loop to one of the jejunal diverticula. Resection of diverticulae bearing jejunal loop and end-to-end single layered anastomosis was performed. Patient had poor nutritional status (albumin 2.1 g/dl) and was put on partial parenteral nutrition for 3 days. Wound was allowed to heal by second intention, as subcutaneous - skin layers were not closed. Patient was discharged on POD 7 . He was followed up on OPD basis on alternate days till wound healed and then on a monthly basis. He was well in the sixth month. Histopathology of resected portion of jejunum revealed multiple diverticulae with acute and chronic inflammatory reaction in all layers. Serosa and periserosal fatty tissues around the diverticulae show areas of prominent acute exudative inflammatory infiltrate [Figure - 3]. Discussion Among small bowel diverticulosis, the diverticulosis of jejunum is rare. It has been reported in approximately 0.06 - 1.3% of autopsies, and up to 0.42% in roentgenographic studies of the small bowel.[3] Harris et al. (1997) reported incidence of jejunal diverticulosis in the general population from 0.02 to 7.17%, where most of the persons were asymptomatic and only 10% developed complications.[4] The presentation of jejunal diverticulosis is in the sixth or seventh decade of life.[3] The patient in this study was in his sixth decade (55 years). Enteroliths, the endogenous foreign bodies were first of all described by Pfahler and Stamm in 1915, but enteroliths causing ileus similar to gallstone ileus was first reported in 1921 by Philips. He noted the difference in chemical composition of both and found that the enteroliths contained unconjugated choleic acid with little or no cholesterol, whereas gallstones usually contained cholesterol and bile pigments.[5] The maximum size reported in the literature is more than 6 cm, and maximum number is up to 1400 enteroliths proximal to a postoperative stricture in a patient who had surgery for colon carcinoma.[5] The enteroliths size in this case was 5 x 4 cm. [Table - 1] shows the various causes that have been implicated in the formation of enteroliths. Most of these conditions lead to stasis or hypermotility.[5] The other conditions that can produce a similar clinical presentation of small bowel obstruction are a food bolus or bezoars (false enteroliths).[6] Surgical treatment of enteroliths obstruction has to be planned if conservative treatment with decompression of the gastrointestinal tract, rehydration, and correction of electrolyte imbalances fails. Milking of enteroliths distally into colon, crushing, or enterotomy and stone extraction are adequate in most of the cases. [1],[2],[3],[4],[5],[6],[7],[8] In a few cases, milking distally is not possible[1],[6],[7] and if there is diverticulosis, bowel perforation or multiple diverticuli over a limited portion of gut, then resection and anastomosis, or laparoscopic-assisted small bowel resection are indicated.[5],[6] In this case, the subject presented with features of small and large bowel obstruction as well, due to adhesion band extending from one of the diverticulae to the sigmoid colon loop. Recognition of the entity and resection of the diverticulae-bearing segment of jejunum with end-to-end anastomosis was curative. Conclusion Small bowel obstructions secondary to an enteroliths formed in the duodenal or jejunal diverticulum is a rare complication. Only 34 cases are reported in literature. The large-bowel and small-bowel obstruction presenting together has not been mentioned in the literature; this condition could only be diagnosed at laparotomy and treatment was curative and effectiveReferences
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05067f1.jpg] [is05067f2.jpg] [is05067t1.jpg] [is05067f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}