 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
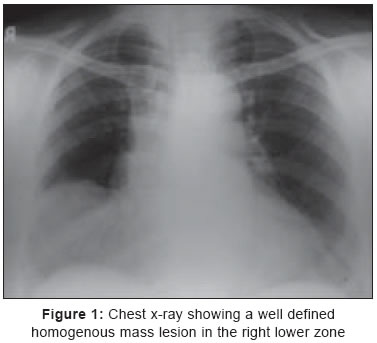
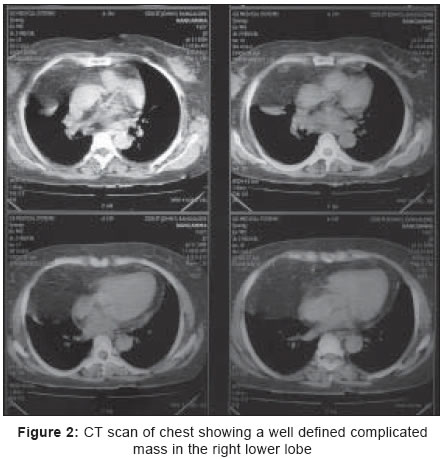
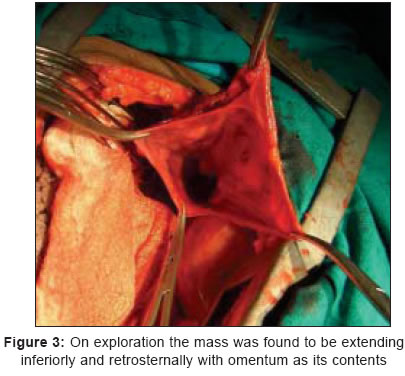
Indian Journal of Surgery, Vol. 67, No. 4, July-August, 2005, pp. 222-223 Case Reports Morgagni's hernia: An unusual presentation Rajaram BV, Srikrishna SV Department of Cardiothoracic Surgery, St Johns National Academy of Health Sciences, Bangalore, Code Number: is05068 Abstract Morgagni's hernia is an uncommon type of diaphragmatic hernia which could be diagnosed with an ultrasound or CT scan. Rarely, the diagnosis may not be obvious until the surgery. We present one such case which mimicked a pulmonary mass lesion, but was detected to be a Morgagni's hernia intraoperatively and managed effectively.Keywords: Morgagni′s, Diaphragmatic, Hernia Morgagni′s hernia is a rare type of diaphragmatic hernia in which abdominal contents herniate into the thoracic cavity through the defect between the xiphoid and costochondral attachments of the diaphragm. We present an unusual encounter with a Morgagni′s hernia that eluded an accurate preoperative diagnosis. Case History A sixty-two year old obese postmenopausal lady presented with a three month history of breathlessness. The breathlessness was of insidious onset that gradually worsened over three months. She had no history of chest pain, palpitation, cough, hemoptysis or fever. She had no abdominal symptoms. On examination, she was tachypnoeic, but the rest of her vitals were normal. There was decreased air entry in the right basal region but no adventitious sounds were heard. Examination of her cardiovascular and abdominal systems was normal. Her chest x-ray showed a well defined homogenous mass lesion in the right lower zone [Figure - 1]. Ultrasound and CT scan [Figure - 2] of her chest revealed a well defined complicated mass in the right lower lobe suggestive of a hydatid cyst. No intra-abdominal pathology was detected in either investigation. A working diagnosis of a mass lesion in the right lower lobe of the lung, most probably a hydatid cyst was considered, and an exploratory right lateral thoracotomy was done. At thoracotomy, a large fat pad was seen in the right cardiophrenic angle. Following dissection of this fat pad, a well-circumscribed mass was found under it. On dissection the mass was found to be extending inferiorly and retrosternally. A diagnosis of Morgagni′s hernia became clear [Figure - 3]. The sac was opened to reveal omentum as its contents. Omentectomy and excision of the sac followed by primary repair of the defect was done. Postoperatively, the chest x-ray showed well expanded lung fields and no residual mass. In the brief 6 month follow up period the patient is asymptomatic and doing well. Discussion Morgagni′s hernia is a rare congenital diaphragmatic hernia, the incidence of which has been reported to be less than 5% of all diaphragmatic hernias.[1] It is more common on the right side due to extensive pericardial attachment to the diaphragm on the left side. Though congenital in origin, it usually presents in the middle aged and is more common in the obese.[2] The patients are usually relatively asymptomatic and the lesions are commonly detected on a plain x-ray. The diagnosis is confirmed with a CT or ultrasound or by contrast studies and can be managed effectively by a transabdominal approach.[3] Nakamura et al.,[4] have shown that a MRI can detect the transthoracic herniation of contents, thereby confirming the diagnosis in doubtful cases. Though conservative approaches have been advocated,[5] obstruction is known to occur and, therefore surgical repair is advocated by most surgeons. In summary, the importance of Morgagni′s hernia lies in the difficulty in clinical diagnosis in some cases; it often mimics many other intrathoracic conditions and goes unrecognized until surgery. If the possibility of Morgagni′s hernia is kept in mind, its clinical recognition becomes relatively simple and facilitates an effective cure. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05068f3.jpg] [is05068f2.jpg] [is05068f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}