 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
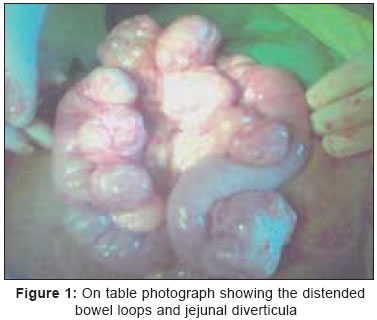
Indian Journal of Surgery, Vol. 67, No. 4, July-August, 2005, pp. 224 Images in Surgery Intestinal obstruction due to multiple jejunal diverticula Alam Shabbir, Manoj Bobby DV, Balu K Department of General Surgery, Kasturba Medical College, Manipal Academy of Higher Education, Mangalore-575001, Karnataka Code Number: is05069 An elderly female with upper GI obstruction clinically and radiologically, underwent exploratory laparotomy which revealed grossly dilated proximal jejunal loops with multiple diverticula on the mesenteric side and bowel wall thickening [Figure - 1]. Resection and anastamosis was done. 'Jejunal diverticulosis and its complications′ is a rare surgical disease with an incidence of 1.1 - 2.3% (together at enteroclysis, at laparotomy and autopsy).[1] Incidence increases with age (M:F = 2:1). Jejunal diverticula occur on the mesenteric border at the sites of perforation of muscle layer with blood vessels. The mechanisms of occurrence include-
60 - 70% are asymptomatic; found incidentally at laparotomy or at contrast studies. 10 - 20% present acutely with: diverticulitis (+/- abscess), perforation, massive GI haemorrhage, intestinal obstruction. Chronic sympatomatology includes vague chronic abdominal pain, malabsorption syndrome, functional pseudo obstruction and chronic low grade GI haemorrhage. Intestinal obstruction can be functional pseudo-obstruction or mechanical. Mechanical obstruction can be due to inflammation associated with diverticulitis/stricture/adhesions, pressure on intestinal wall from distended diverticula, intusussception, volvulus, enteroliths developed within diverticula (getting impacted locally or distally after getting dislodged from diverticula).[1] Majority of the symptomatic patients require resection of the affected segment and end to end anastamosis. Exceptions to this are - multiple diverticula scattered over the small bowel, in which case, resection should be limited to the segment with largest diverticula. Also, in obstruction due to enterolith, an enterotomy / caecotomy (to milk and remove the enterolith through caecum) is done.[1] Malabsorption syndrome is treated initially with antibiotics which may or may not be followed by surgery. Asympatomatic patients can be kept on follow up and observed. Laparoscopic resection and anastamosis is also being performed for diverticulitis References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05069f1.jpg] |
| |||||||||

{kind=link}