 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
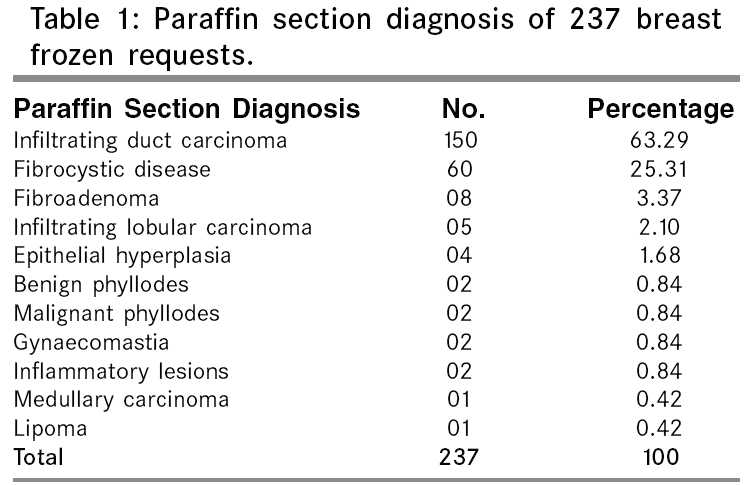
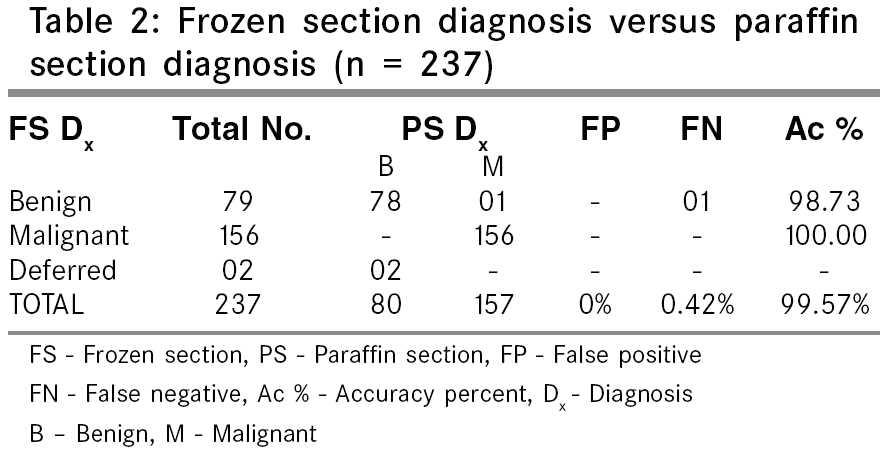
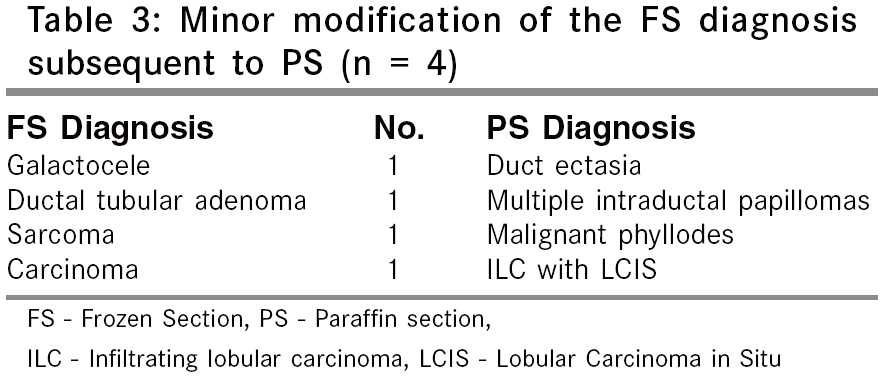
Indian Journal of Surgery, Vol. 67, No. 5, September-October, 2005, pp. 248-252 Original Article Role of frozen section evaluation in patients with breast lumps: A study of 251 cases Karve PV, Jambhekar NA, Desai SS, Chinoy RF Department of Pathology, Tata Memorial Hospital, Parel, Mumbai - 400 012, India Code Number: is05077 Abstract Context: Frozen section is an invaluable intra-operative tool for evaluation of breast lumps.Aims: The aim of this study was to (1) calculate the overall accuracy, false positivity, false negativity for frozen section of breast lumps, (2) analyze the causes of discrepancies, and (3) compare the data with that of published literature on frozen section of breast lumps. Material and Methods: Two hundred and fifty one frozen sections comprising 237 breast lumps, 10 axillary nodes and 4 lumpectomy margins received for frozen section in 1997 were analyzed. Pathology reports and slides (of both frozen and paraffin sections) were reviewed. The values were calculated using paraffin slides as the gold standard. Results: The 237 lumps received for primary diagnosis comprised 157 malignant and 80 benign lesions. The false negativity rate was 0.42%, false positive rate 0%, deferral rate 0.84%, overall accuracy rate was 99.57%. The false negative diagnosis was an error of interpretation. False negativity rate for axillary nodes was 20% and accuracy was 80%. Accuracy for margins was 100%. Conclusion: Frozen section has a role despite the raging popularity of aspiration cytology in the following settings: (1) Difficult cytology (2) Evaluation of lumpectomy margins. (3) Intra-operative nodal status. Keywords: Frozen section, breast, accuracy, utility One of the earliest organs to be studied by frozen section in the year 1891[1] was the breast. Since then, frozen section has been an invaluable and a popular tool for intra-operative evaluation of breast lumps. More recently, Fine Needle Aspiration Cytology (FNAC) has diminished the demand for frozen section evaluation of breast lumps. Yet in certain situations, particularly when FNAC fails, the need for frozen section persists. The aim of this study was to analyze the indications for frozen requests on breast lumps and also to determine the accuracy, false positivity and false negativity of this method of diagnostic evaluation. The results have been compared with published literature and the role of frozen section diagnosis for breast lumps has been reassessed in the present scenario. Material and Methods A retrospective analysis of frozen sections on 237 breast lesions, 10 axillary nodes and 4 lumpectomy margins together comprising 10.99% of the total 2220 frozens performed in the year 1997 was done. On receipt in the frozen laboratory, the breast specimens or the lymph nodes were examined grossly. The size of the breast lesions, their shape, circumscription, colours, consistency, and presence of necrotic, haemorrhagic or cystic areas were noted. Each node was bisected and the abnormal looking hemi-section was processed for frozen section. To evaluate the margins of a lumpectomy specimen, the closest margin(s) were selected, inked and frozen. The most representative tissue slice measuring about 1cm x 1cm x 0.3cm was processed in an open door cryostat at a temperature of -23°C. Sections measuring 5m in thickness were cut and toluidine blue staining and rapid hematoxylin and eosin (H & E) staining were performed. After the frozen section diagnosis was rendered, the frozen tissue was thawed to room temperature and fixed in formalin overnight for further paraffin processing. The unfrozen remaining tissue was also transferred to formalin for paraffin embedding. The H & E stained actual frozen section slides on which the diagnosis was rendered and the subsequent paraffin embedded tissue sections were together evaluated with an emphasis on studying the paraffin processed sections of the tissue actually frozen. The lesions were classified as fibrocystic disease, fibroadenoma, inflammatory lesions, and malignancies; the latter were further sub-classified wherever possible. The following terms were used for describing the accuracy rates[2]- True Negative True Positive False Positive False Negative Accuracy (%) = True Positive + True Negative x 100 The term deferred included the category "Await paraffin section". Results In the following write-up, the observations on the breast lumps precede those on the margins and the nodes. Out of the 237 breast lesions received for a primary diagnosis, 157 were malignant and 80 were benign. [Table - 1] shows the paraffin diagnoses of 237 breast lesions. As expected, the maximum frozen requests (63.29%) were for lumps diagnosed ultimately on paraffin sections as infiltrating duct carcinoma whereas one-fourth were on lumps subsequently diagnosed as fibrocystic disease of the breast. Only 2.10% were for lobular carcinoma. This represents the general pattern of accession of breast lumps in the pathology laboratory. On comparing the frozen section diagnoses with paraffin section diagnoses [Table - 2], it was found that there were no false positives, 0.42% false negative results and the rate of deferral was 0.84% [2 cases]. The accuracy for benign lesions was 98.73%, for malignant lesions it was 100%, and the overall accuracy was 99.57%. Both the deferred diagnoses were labeled as fibrocystic disease with epithelial proliferation. A single false negative diagnosis occurred due to an error of interpretation, wherein an infiltrating lobular carcinoma was mistaken for fibroadenomatoid hyperplasia on frozen section. Minor modifications of the frozen diagnosis were necessary in four cases as shown in [Table - 3]. However, these modifications subsequent to paraffin section had no bearing whatsoever on the further management of the patient. The margins of four lumpectomy specimens were received for frozen section evaluation. All 4 were negative on frozen section and confirmed on paraffin section [accuracy 100%]. Samples of ten axillary lymph nodes, one each from 10 patients, were received for frozen section. On frozen section only 2 out of these 10 nodes were positive for metastasis whereas on paraffin processing, 2 additional nodes showed metastasis and 6 remained negative. Thus, metastatic deposits in 2 nodes were missed on frozen; the false negativity rate was 20%, false positivity rate was 0%, and the overall accuracy was 80%. Discussion Breast carcinoma is the second most common malignant tumor among rural Indian women after carcinoma cervix whereas in urban Indian women, breast carcinoma overcomes the incidence of carcinoma cervix. Frozen section is useful for obtaining diagnosis of a breast lump, axillary nodes, and lumpectomy margins. FNAC is a simple, cheap technique, which is utilized much more frequently in the evaluation of breast lumps, and axillary nodes; yet the need for frozen section evaluation is felt in the following situations:
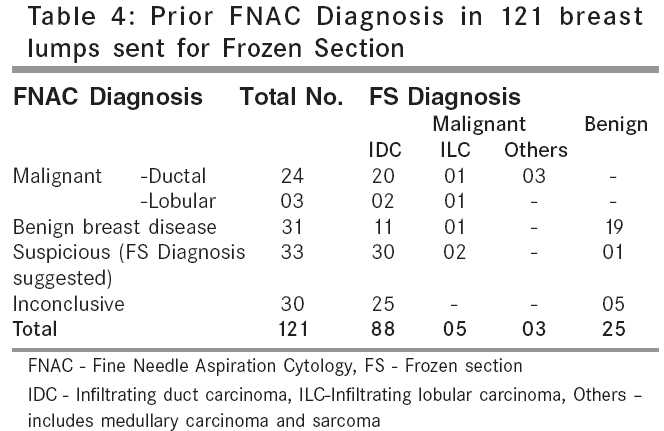
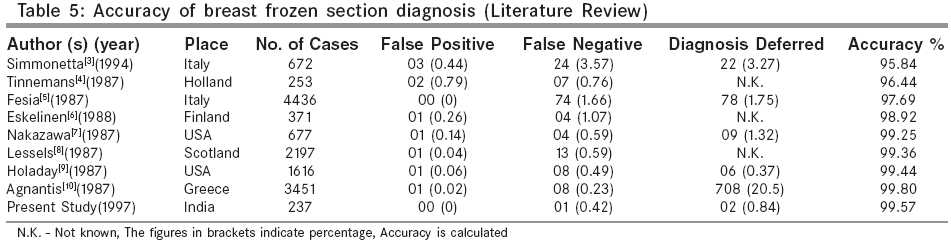
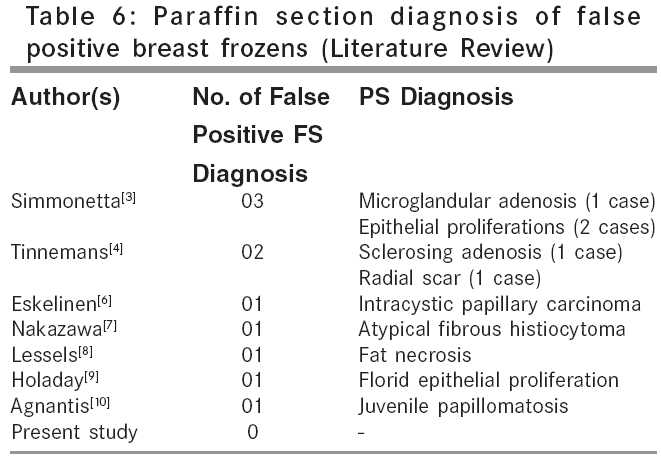
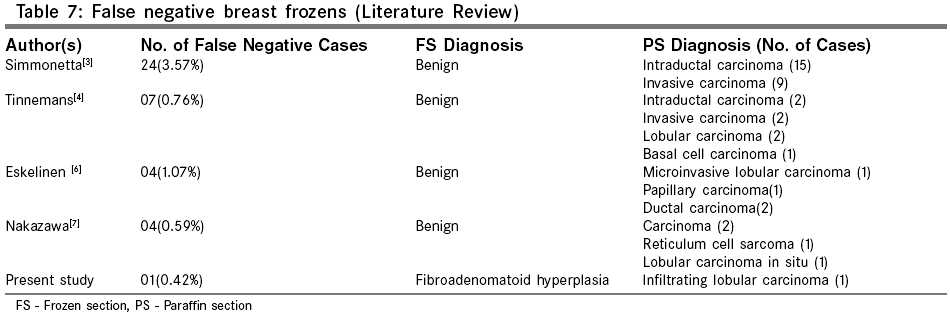
In the present study, 51 % of frozen sections on breast lumps were requested despite earlier FNAC evaluation as shown in [Table - 4]. One-fourth of the FNACs were suspicious for malignancy for which tissue diagnosis was suggested and another one-fourth were inconclusive. In both the above situations frozen was essential. Again distinction between low grade ductal and a lobular carcinoma is difficult on FNAC and it is important for therapeutic decisions. On analysis of the published data on frozen section of breast lumps between 1976 and 1997, [3],[4],[5],[6],[7],[8],[9],[10] the accuracy rate was found to be between 95.84% to 99.8%, false positivity rate between 0% to 0.79%, false negativity rate between 0.23% to 3.57%, and the rate of deferral was between 0.37% and 20.5% [Table - 5]. Analysis of the present study revealed an accuracy rate of 99.57%, false positivity rate 0%, false negativity rate 0.42% and the rate of deferral as 0.84%, well within the range reported in literature. Evidence from literature shows that the benign lesions which were frequently over diagnosed as malignancy on frozen section included microglandular adenosis[3], epithelial proliferations,[3],[9] sclerosing adenosis[4], radial scar,[4] intracystic papilloma,[6] juvenile papillomatosis[10] and fat necrosis[8] as shown in [Table - 6]. Microglandular adenosis is a poorly circumscribed glandular proliferation in a collagenous stroma; it is known to simulate malignancy.[3] Presence of colloid like material within open lumina and absence of nuclear atypia points towards its benign nature.[11],[12] Epithelial hyperplasias are also mistaken for malignancy. [3],[9] Tavassoli and Norris[13] emphasised that the cytologic appearance is more important feature in distinguishing atypical hyperplasia from ordinary hyperplasias. When the cytologic features of intraductal carcinoma are present in an otherwise usual localized ductal hyperplasia, the lesion is diagnosed as atypical ductal hyperplasia.[13] Sclerosing adenosis is best diagnosed under a scanner lens. Lobulo-centricity, a regular basement membrane around each glandular space and a two-cell layer favor a diagnosis of sclerosing adenosis.[14] Although clinically radial scars are non-palpable small lesions detected incidentally, microscopically they can be mistaken for malignant lesions[4] especially when the spindle cell and inflammatory component is conspicuous and scarring is less.[14] Papillomas, both solitary and multiple, may undergo infarction and extensive sclerosis; this in turn can produce frightening distortion and patterns which can lead to an over diagnosis of carcinoma. However, blandness of epithelial proliferation is an important feature to recognize. The confident distinction between a papilloma and a papillary carcinoma on frozen section is difficult and according to some should not be attempted till paraffin section is ready.[15] The present study did not reveal any false positive diagnosis on frozen section. The malignant lesions which are commonly under-diagnosed as benign (literature review) are listed in [Table - 7]. The single false negative entity in the present study was an infiltrating lobular carcinoma on paraffin sections. As seen in [Table - 7], amongst the 16 cases (including present study) in publications comprising lobular carcinoma,[4],[6],[7] 5 false negatives were finally diagnosed as lobular carcinomas (5 out of 16 = 31.5%), and out of the total 40 false negatives enlisted, 19 were intraductal carcinomas. This table emphasizes that invasive lobular carcinoma and intraductal carcinoma are the two most frequently under-diagnosed lesions on frozen section. The presence of intra-cytoplasmic lumina within the proliferating cells and their pagetoid growth pattern within the involved ducts favors a diagnosis of lobular neoplasia.[16] Intraductal carcinoma is an intraductal proliferation of monotonous cells, with hyperchromatic, round or oval nuclei forming regular spaces, rigid geometric configuration and no swirls or streaming.[17] The incidence of false negativity on frozen tissues increases with diminishing size of the lesion,[6] due to artifactual distortion on freezing, and the apprehension about lack of adequate tissue for paraffin section. Hence the Association of Directors of Anatomic Surgical Pathology recommends that lesions less than 1cm should not be frozen.[18] A review of the literature has shown that the lesions most commonly deferred are intraductal carcinomas,[3], [10] intraductal papillomas,[9],[10] epithelial hyperplasia,[3] and lobular carcinoma in situ.[10] We recommend that ductal hyperplasias, which appear cytologically atypical but do not reveal either gross or convincing microscopic features of carcinomas, should be deferred. With the increased popularity of breast conservation therapy and limited axillary node dissection there have been increasing requests for frozen section of margins of lumpectomies and axillary nodes. We received four breast lumps for lumpectomy margins. All margins were negative and the accuracy was 100%. A study published on frozen section of breast margins report an accuracy of 87%.[19] In the present study, there were 10 requests for axillary node sampling. There were no false positive diagnoses. The false negativity rate was 20 % [2 cases] which is unacceptably high due to microscopic metastasis. Step sectioning at frozen,23 and assessment of entire node including adipose tissue,23 trisection of the node23and immunohistochemistry at frozen for detection of micrometastasis[22] have all been recommended to improve the diagnostic accuracy of frozen section. Literature published on axillary node analysis by frozen has shown accuracy rates of 92.08%,[20] 95.58%,[21] 96.29%[22] and false negativity rates of 8%, 4.5%, 3.8% respectively in studies comprising 88, 68, 54 cases respectively. In the years subsequent to that of the present analysis 1997, there has been a steady increase in the frequency of requests for sentinel node analysis by frozen section and the decision for an axillary dissection depends on the status of the sentinel node. Confirmation of breast malignancy with frozen section on a needle core biopsy and assessment of ER/PR status on paraffin is being increasingly sought before starting chemotherapy. To conclude, despite increasing popularity and undisputed utility of FNAC, there will be situations where frozen section still stands out as the method of choice for rapid diagnosis. Only in those few conditions where frozen section fails to provide a conclusive diagnosis, will the final paraffin section be needed to accurately arrive at a definitive diagnosis. A judicious selection of one or more of these modalities is required in every patient presenting with a suspicious breast lump. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05077t3.jpg] [is05077t5.jpg] [is05077t2.jpg] [is05077t1.jpg] [is05077t7.jpg] [is05077t6.jpg] [is05077t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}