 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
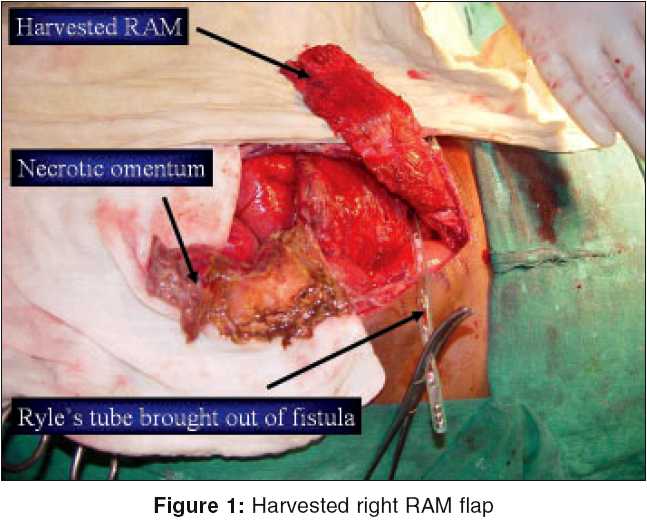
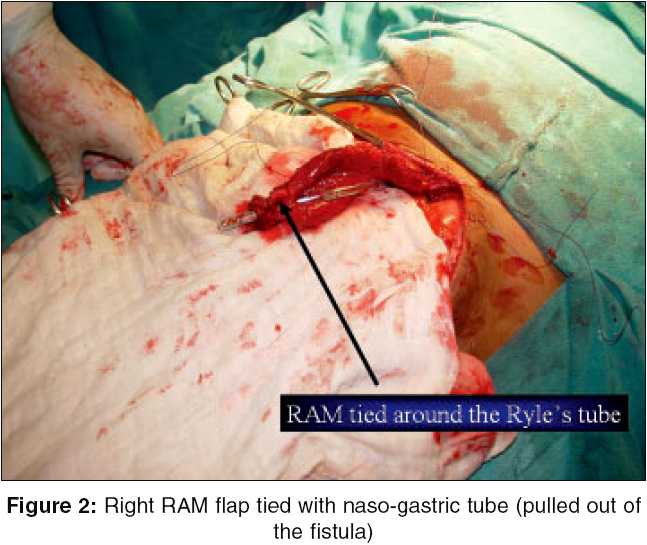
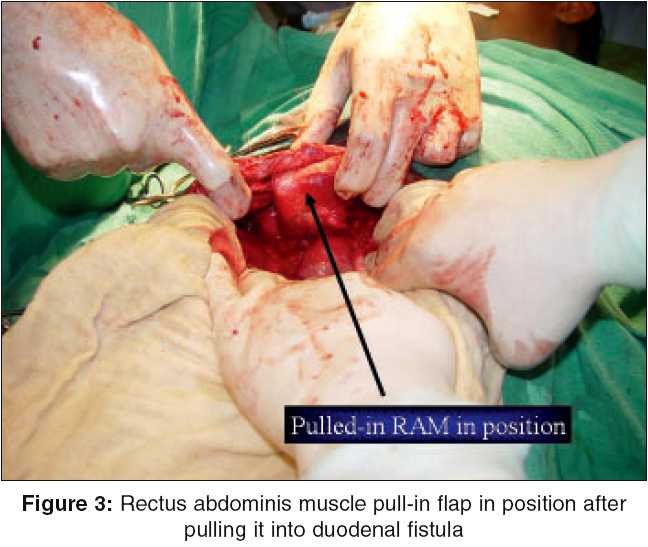
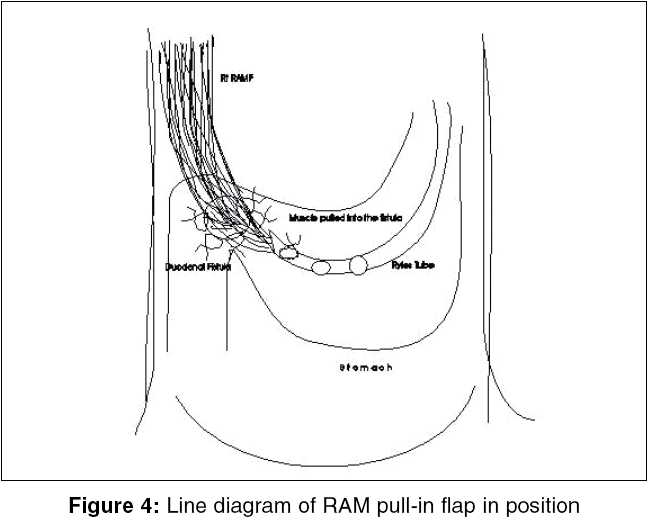
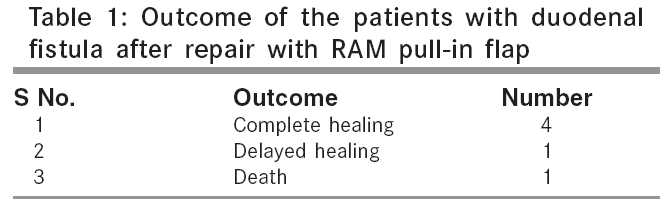
Indian Journal of Surgery, Vol. 67, No. 5, September-October, 2005, pp. 253-256 Original Article Repair of duodenal fistula with rectus abdominis muscle 'pull-in' flap Agarwal P, Sharma D Plastic and G-I Surgery* units, Department Of Surgery, Netaji Subhash Chandra Bose Government Medical College, Jabalpur - 482 003 Code Number: is05078 Abstract Objective: Large duodenal fistulae are difficult to repair, due to complex duodenal anatomy. Musculoepithelial flaps are conventionally used for reconstruction of large soft tissue defects. This is the first study reporting clinical use of rectus abdominis muscle (RAM) pull-in flap for repair of duodenal fistulae.Materials and Method: Six patients of duodenal fistulae (resulting from leakage of peptic perforation repair) underwent repair using right RAM pull-in flap, based on superior epigastric artery. Rectus abdominis muscle flap, after being harvested, was tied to naso-gastric tube (brought out of duodenal fistula) that was then pulled back in the stomach. Muscle was then anchored to the edges of duodenal fistula with few interrupted 2-0 vicryl sutures. Results: Duodenal fistulae healed within 3-5 days in all the cases except one, in which some bile continued to leak for 20 days. One patient died within 12 h of second surgery. Discussion: Rectus abdominis muscle pull-in flap for closure of duodenal defect is a simple, technically easy and dependable procedure, which can be performed, quickly in critically ill patients. It can be used for repair of a large duodenal defect with friable edges when omentum is not available or when other conventional methods are impractical. Keywords: Duodenal fistula, rectus abdominis muscle flap Large duodenal defects/fistulae are technically difficult to repair and associated with high morbidity and mortality. The reasons for disruption of duodenal closure after tissue loss are duodenum′s complex anatomy, marginal blood supply shared with pancreas, high intraluminal pressure, tendency of mucosa to extrude through suture line, break down from autodigestive enzymes of pancreas and bile. Such duodenal fistulae have been conventionally dealt with by closure with omental implantation or patch, falciform ligament, jejunal serosal patch technique, Roux-en-Y duodenojejunostomy, exclusion or diverticulization of duodenum, including partial gastrectomy or gastric dissociation.[1] In a re-do operation, omentum may not be available and in a seriously ill patient, it is neither feasible nor advisable to perform major time consuming surgical procedures like partial gastrectomy, serosal patching, or Roux-en-Y duodenojejunostomy. This led us to devise and use rectus abdominis musculo-peritoneal (RAMP) flap successfully in such cases.[2] We now submit a simplification of the technique in the form of rectus abdominis muscle (RAM) pull-in flap. Materials and methods Institutional ethics committee approval was obtained and this study was conducted on six patients of duodenal fistulae resulting from leakage after peptic perforation repair, from June to December 2004. These patients had perforation in the first part of duodenum, which was primarily repaired by mid-line incision using Graham′s omentopexy, but duodenal fistula developed within 48-72 h postoperatively. Informed consent was taken and patients were re-explored through the same incision within 48 h of detection of leakage and duodenal fistula located. Right RAM was separated from anterior and posterior rectus sheath and detached from lower end and laterally [Figure - 1]. A nasogastric tube was passed and it was taken out through duodenal fistula. Harvested rectus muscle was than pulled in to the fistula after tying it to nasogastric tube with 2-0 chromic catgut stitches [Figure - 2][Figure - 3][Figure - 4]. This muscle was then anchored with 2-0 vicryl-interrupted sutures to the edges of fistula. Feeding jejunostomy was added and a tube drain was kept next to the closure and brought out of the right flank. Depending upon the degree of peritoneal contamination, abdomen was closed in layers (in 2/6 patients) or left open as a laparostomy (in 4/6 patients). Because of infrastructural and financial constraints, none of the patients received ventilatory support or TPN. All patients received third generation cephalosporin, aminoglycoside and metronidazole to control the associated infection/septicemia. Parameters looked for postoperatively were those of sepsis induced multiple organ failure and amount of bilious discharge through the right flank drain. Healing was judged by cessation of bilious fluid in the drain. All the patients were followed up for at least 6 months; to look for gastric outlet obstruction. Results The study included six male patients. All had developed fistula after 3-5 days of closure of peptic perforation in our hospital. Age of the patients ranged from 30 to 50 years. All the patients were poorly nourished (weight 40-50 kg and Hb less than 10 gm%) and presented late after the primary event, which ranged from 2 to 4 days after the onset of peritonitis. Duodenal fistulae healed within 3-5 days in four cases. Delayed healing occurred in one case, in which some bile continued to leak for 20 days. One patient died within 12-24 h of second surgery due to pre-existing sepsis induced multi organ system failure (MSOF) [Table - 1]. Gastric outlet obstruction was not seen up to 6 months after surgery. Discussion Duodenal perforations are routinely closed with omental patch or its modifications like omental plug or pull in. [3],[4],[5] In most cases the repair rarely leaks, but when it fails, it forms a high output duodenal fistula, which leads to profound derangement of ′milieu internale,′especially if the presentation is late with presence of preoperative shock, patient is in the older age group or there are concomitant medical problems.[6],[7] In such a precarious situation, it is neither feasible nor advisable to perform major surgical procedures like partial gastrectomy, serosal patching, Roux-en-Y duodenojejunostomy; as all these procedures are not only time consuming, but demand a level of surgical skills which may not be available in an emergency setting.[4] Conventional wisdom dictates that healthy vascularized tissue should be incorporated in the repair of any defect with tissue loss or with friable edges. Therefore, in redo cases where omentum is not available or the cases where repair with omentum fails, we have earlier used RAMP flap, which found peer acceptance,[2] RAM pull-in is a simplification of this technique. There are many advantages of this modification:
The use of a vascularized flap augments the blood supply to the diseased area, thereby hastening the healing process and counters the infection in much better way. It is assumed that myoglobin released from muscle is also a contributory factor in wound healing.[8],[9] Experimental work has shown that re-epithelialization occurs over the pulled-in muscle from the edges of defect and metaplastic adaptation of epithelium in to neomucosa takes place by 8-12 weeks.[10],[11] Rectus abdominis has a constant and reliable vascular pedicle, making its use a popular and versatile flap. As the pedicle of superiorily based flap enters high up in the abdomen, there is no risk of bowel loop twisting around this flap and causing obstruction; inferiorly based flap is avoided for this reason. Success depends upon maintaining the adequate arterial supply and venous drainage of muscle so it can withstand the digestive properties of the duodenal contents for a period long enough to permit healing.[12] We have successfully used right RAM flap for surgical closure of duodenal fistulae in six patients, however, in case of right para-median incision having been used for the earlier exploration, left RAM can be used. In our study, all patients had high output fistula with poor nutritional status. In addition, all patients had reported late after the onset of peritonitis (2-4 days) by which time the peritoneum and bowel were severely inflamed. Despite the presence of poor prognostic factors, the RAM pull-in flap was successful in closing the fistula in 5/6 cases. One patient developed minor leak (output < 200 ml/day), which healed on conservative treatment, probably significant bulk of muscle ensured that leaking fistula remained low output and inflammatory adhesions between duodenum and the muscle flap prevented breakdown at the fistulous site. One patient died due to pre-existing septicemia and MSOF as it occurred within 12 h of surgery. Four patients in our series underwent laparostomy, which ensures drainage of residual sepsis; allows daily inspection of the status of flap and helps in early detection of bile leak. In cases of leakage, all the bile comes out of the peritoneal cavity thus reducing the chances of bile peritonitis. We routinely added feeding jejunostomy in all our patients; as it shortens the time to resumption of feeds and is a useful adjunct to repair of a difficult duodenal perforation. Four (out of six) cases we did under monitored care (monitoring by anesthetist) local anesthesia. This helps in reducing the anesthesia-related morbidity and mortality because these patients were already critically ill. Conclusion Rectus abdominis muscle flap is a robust flap, which can withstand the digestive activity of the duodenal contents and encourages healing due to its good blood supply. Using RAM pull-in flap for closure of duodenal defect is a simple, technically easy and dependable procedure, which can be performed, quickly in critically ill patients. This technique can be easily used in large duodenal fistulae with friable edges when omentum is not available or when other conventional methods are impractical.References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05078f3.jpg] [is05078t1.jpg] [is05078f1.jpg] [is05078f4.jpg] [is05078f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}