 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
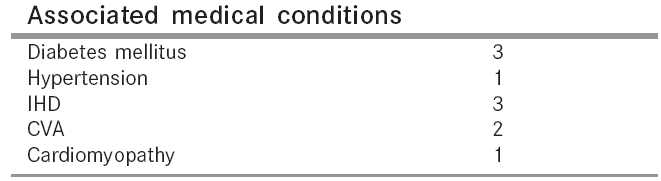
Indian Journal of Surgery, Vol. 67, No. 5, September-October, 2005, pp. 257-259 Original Article Acute nontraumatic upper limb ischaemia: A protocol for management Vinayagam K, Arumugam S, Rao UV, Vidyashankar S Department of Vascular Surgery, Manipal hospital, 98, Rustom Bagh, Airport road, Bangalore - 560017, India Code Number: is05079 Abstract Aim: To determine the role of different modalities available and draw guidelines for the treatment of acute ischaemia of the upper limb.Materials and Method: This is a retrospective study carried out over a period of 7 years between 1994-2000 comparing embolectomy with thrombolytic therapy for upper limb ischaemia. Twenty-two patients presenting with acute upper limb ischaemia admitted in this hospital were studied. Their age, sex distribution, symptoms and associated medical illnesses were documented. Pain was the predominant symptom in most of them. The underlying causes were treated accordingly in the form of excision of cervical rib or high first rib, angioplasty and stenting. Results: The overall success rate was 91% (n = 20) with an amputation rate of 9%. In the surgical group (ten patients), seven patients responded well. Two patients recovered with further thrombolytic therapy. One patient underwent amputation. In the thrombolytic therapy group (ten patients), six patients responded to thrombolytic therapy alone. The rest of them recovered with further embolectomy. Conclusion: Thrombolytic therapy can thus be the first modality of treatment for acute nontraumatic upper limb ischaemia if the limb is viable. Keywords: Acute ischaemia, upper limb, thrombolytic therapy, amputation Upper limb ischaemia is uncommon when compared to that in lower limb. It poses diagnostic and therapeutic challenge because of the multiple causes and poorly understood disease process. Timely management of acute upper limb ischaemia is important because the consequences can be devastating due to loss of limb or impairment of function. Sometimes it may also result in loss of life. There is considerable controversy about how aggressively acute arm ischaemia should be treated particularly when the arm appears viable.[1] Fewer than 50 publications exist and there are no randomized trials. Surgery has been the standard treatment for over a century. Though peripheral thrombolysis is well established in the management of lower limb ischaemia, there are very few papers published explaining its role in upper limb ischaemia. It is associated with a 10% risk of hemorrhage, which may require blood transfusion, may need an operation or may die from bleeding. The aim of this study is to determine the role of different modalities of treatment available and draw guidelines for the treatment of upper limb ischaemia. Patients and methods This study was carried out over a period of 7 years between 1994 and 2000. A total number of 22 patients were studied who presented with acute upper limb ischaemia [< 2 weeks] who were admitted and treated as inpatients. A 59% of them were females and 41% were males. Their age ranged from 21 to 70 years with an average of 45.5 years, 55.5% belonging to the group between 40 and 60 years. Fifteen patients presented with pain, which was the predominant symptom. Pain was associated with discoloration in two patients. Weakness and tingling was present in two patients. One patient came with Raynaud′s phenomenon. All had signs of ischaemia, eight of them had other associated medical conditions as shown in the table. Routine investigations were carried out in all patients including coagulation profile. Five were worked up for collagen vascular disease and one was positive for anticardiolipin antibody. Chest and neck x-ray was done in all patients. It revealed cervical rib in two and suspected high first rib in one patient. Angiography was done in all the patients. Sub clavian artery was the site of occlusion in 50% of the patients ( n = 11). Five each had occlusion of axillary and brachial artery (22.7%). Distal occlusion of the radial and ulnar artery was found in one patient (4.5%). Management Surgery (Embolectomy) Thrombolysis
The duration of treatment however varied according to the response. Patients were monitored for bleeding complications and worsening of symptoms. Check angiogram was taken after 24 and 36 h. Results Surgery group Thrombolytic therapy group Others Discussion Before embolectomy became routine, conservative treatment was the only available treatment. This included heparin, re-hydration, bed rest and treatment of contributing medical conditions such as cardiac failure or dysrhythmia.[1] Embolectomy is the most frequently performed surgical procedure for acute upper limb ischaemia. Occasionally nonviable digits may require amputation. The introduction of a Fogarty′s balloon catheter in 1963 revolutionized the treatment of acute limb ischaemia.[2] This is a retrospective study, which compares embolectomy with thrombolytic therapy. Investigations revealed 32% of patients to have a primary lesion in the subclavian artery due to a cervical rib or high first rib or stenosis who were treated accordingly. In 50% a cardiac source was suspected in view of their age and associated medical conditions. In 4.5% essential thrombocytosis was a possible cause. In the remaining 13.5% the cause was unknown. The success rate in the group who underwent surgery was 70% with an amputation rate of 20% ( n = 2). One of them who underwent amputation was diagnosed to have essential thrombocytosis who had repeated emboli. Satiani et al .[3] and Davies et al .[4] have recommended that surgery be performed as soon as possible after correcting electrolyte imbalance, meanwhile attending to associated medical conditions. In advanced ischaemia, embolectomy has been recommended to enable a more distal amputation, but this carried the risk of reperfusion injury and myoglobinuria. More embolectomies can be performed under local anesthesia. [5],[6],[7],[8]Sachetello et al .[9] and more recently others[10],[5],[8] have advised exposure of the bifurcation of the brachial artery to allow direct embolectomy of the radial and ulnar artery. The result of embolectomy is commonly assessed clinically by observing restoration of the radial and ulnar pulses. Treatment of underlying cause is important in the form of excision of cervical rib, angioplasty and stenting. In the thrombolytic therapy group, the success rate was 60% with initial thrombolysis. However, four patients who failed to responds, improved with embolectomy later. None underwent amputation. The explanation for this could be that thrombolysis can lyse the embolus partially and makes embolectomy easier. Earlier all the patients were subjected to embolectomy. With the introduction of peripheral thrombolysis, this was the initial treatment preferred. Though peripheral thrombolysis is well established in the management of lower limb ischaemia, there are very few reports explaining its role in upper limb ischaemia.[11] Catheter directed thrombolysis is based on the principle that activation of fibrin bound plasminogen to the active enzyme plasmin is the most effective means of lysing pathologic thrombi. Thrombolytic agents have also been successfully used intraoperatively to improve the outcome of patients with upper limb ischaemia.[12] Some 10% of patients may suffer haemorrhage, which require blood transfusion, may need an operation to stop bleeding or may die from bleeding.[13],[14] Comparing the results of both the groups, though the initial response was better (70%) in the surgical group the amputation rate was higher (20%). Qeinid et al . have concluded that initial thrombolysis has a significant advantage over surgery. STILE investigators have also found that surgical patients have more major amputations than patients who underwent thrombolysis (5.7%).[15] Though the initial success rate was low with thrombolysis (60%) when compared to surgical group the final outcome was good. No amputation was carried out in this group. Successful thrombolysis should be followed by endovascular or open surgical revision of any lesion unmasked after dissolution of the thrombus. Endovascular modalities such as balloon angioplasty with or without stenting can be performed at the conclusion of thrombolysis, usually through the same access site used for the infusion. It may thus avoid the stress of emergency vascular reconstruction. Conclusion Thrombolytic therapy can thus be the first modality of treatment for acute nontraumatic upper limb ischaemia if the limb is viable. It could be the only treatment if successful. It may reveal an underlying lesion, which can be dealt with accordingly. If it fails an embolectomy can still be done. This is similar to that concluded by Burundi et al .[13] Thrombolysis and surgery are however not competing techniques but should be used in a complementary fashion[22]. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05079t1.jpg] |
| |||||||||

{kind=link}