 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
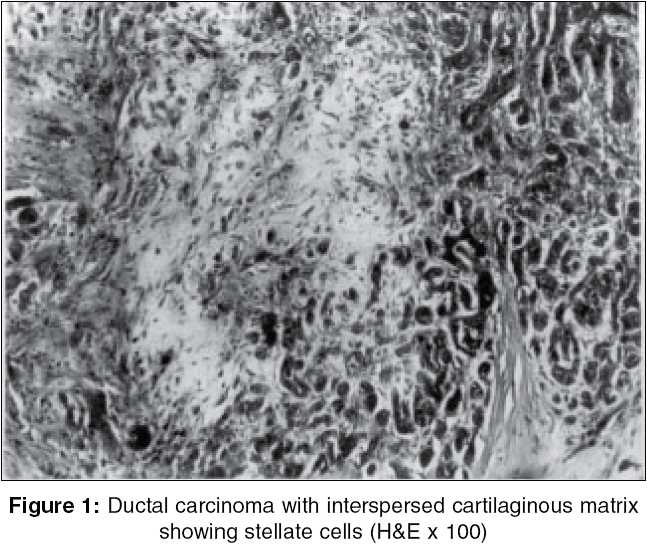
Indian Journal of Surgery, Vol. 67, No. 5, September-October, 2005, pp. 262-264 Case Reports Mammary matrix producing carcinoma - A rare entity Inchara YK, Rajalakshmi T, Makhija P Department of Pathology, St. John's Medical College, Johnnagar, Bangalore, India Code Number: is05081 Abstract Matrix producing carcinoma of the breast is a unique subclass of metaplastic carcinoma, which is characterized by the existence of a ductal carcinomatous component with direct transition to areas showing cartilaginous or osseous differentiation lacking an interspersed spindle cell element. The tumor is of epithelial-myoepithelial histogenesis. It is said to carry a better prognosis compared to other metaplastic carcinomas, despite the presence of heterologous elements, which generally implies an aggressive course. Nodal metastases are also infrequently encountered. This article reports one such rare case in a 46-year-old woman, not just for its' peculiarity at microscopy, but also to highlight its' clinical behavior and hence, the need for its' recognition.Keywords: Breast, matrix producing carcinoma, metaplastic carcinoma Metaplastic carcinomas of the breast encompass a histologically variegated spectrum. Among these, matrix producing carcinoma (MPC) represents a rare and distinctive entity, characterized by the production of abundant cartilaginous and/or osseous stromal matrix but lacking an intervening spindle cell component.[1] The identification of this entity is important to pathologists and surgeons alike, considering its′ superior prognosis to other metaplastic carcinomas. This report highlights one such case, along with a review of current literature and differential diagnoses. Case report A 46-year-old woman presented with a breast lump of 7 months duration with a history of rapid increase in its size, with no pain or nipple discharge. On examination, a firm, mobile 3 x 3 cm, left upper quadrant breast lump was noted. No lymph nodes were palpable. The FNAC of the lump showed features of ductal carcinoma. The patient underwent a modified radical mastectomy. Gross appearance Microscopy Discussion Metaplastic carcinomas are uncommon tumors of the breast, which show cellular components with divergent differentiation and hence, are histologically heterogeneous. They can be divided into five subtypes: MPC, spindle cell carcinoma, carcinosarcoma, squamous cell carcinoma of ductal origin and metaplastic carcinoma with osteoclastic giant cells.[1] Matrix producing carcinomas are characterized by the presence of overt carcinoma with direct transition to matrix-producing cells and osteocartilaginous stroma without an intervening spindle cell component.[1] Wargotz and Norris first described this entity and in their study of 26 cases of MPC, the largest so far, found that the carcinomatous component was moderate to poorly differentiated with a frequent association of intraductal component.[1] The nature of the matrix is variable, ranging from bland cartilage to atypical chondroid to osteoid or overt bone formation. The matrix is made up of acid mucopolysaccharides that stain metachromatically with alcian blue and aldehyde fuchsin and is resistant to pretreatment with hyaluronidase and diastase.[1] In the present case, the epithelial component was a grade 3 infiltrating ductal carcinoma with comedo-DCIS areas and the matrix showed cartilaginous differentiation. Immunohistochemically, reactivity has been noted for keratins, epithelial membrane antigen (EMA), S-100 in all neoplastic cellular elements and also for actin in about half the cases.[1] Keratin and EMA staining is variable within the matrix. Ultrastructural analysis of MPC supports the evidence that the tumor cells are of epithelial-myoepithelial derivation.[1] Myoepithelial cells differentiate along mesenchymal lines and produce a gamut of matrical appearances, as described earlier. These tumors are also known to express CD99/MIC 2, like other chondromyxoid tumors such as mesenchymal chondrosarcoma.[2] Cartilaginous/osseous metaplasia may be uncommonly noted in other mammary tumors, such as Fibroadenoma, Phyllodes tumor, or even Pleomorphic adenoma. The unequivocal presence of carcinoma is a helpful distinguishing feature in such cases. On contrast-enhanced tomography, some of these tumors present a hypodense center corresponding to the acellular matrical core, with ring-like enhancement.[3] This feature may add to the index of clinical suspicion. The finding of axillary lymph node metastases is rare and was not seen in the present case. Huvos et al. observed that the low incidence of nodal metastases in neoplasms with osteochondroid metaplasia did not correlate with subsequent clinical outcome.[4] Mastectomy is said to afford the best protection against recurrence with a 5 years survival rate of about 68%, which is in contrast to rates of less than 55% for metaplastic carcinomas in general and below 50% for grade 3 ductal carcinomas.[1],[5] This is also contrary to the finding that metaplastic carcinomas with a heterologous stromal component carry a worse prognosis.[6] Radiation and chemotherapy were also found to be of limited value.[1] They are usually Estrogen and Progesterone receptor negative.[7] Our patient is currently asymptomatic and is being followed up. In summary, matrix producing metaplastic carcinomas are a distinct subgroup with direct transition from carcinomatous to osteocartilaginous areas and are said to carry a more favorable prognosis than other metaplastic carcinomas. The peculiarity of these tumors are that though they are usually composed of a mixture of high-grade infiltrating duct carcinoma and areas of heterologous stroma, each of which is known to behave aggressively, these composite tumors have a better 5-year survival rate and less frequent nodal metastases. Additional studies are warranted to establish the significance of these findings. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05081f1.jpg] |
| |||||||||

{kind=link}