 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
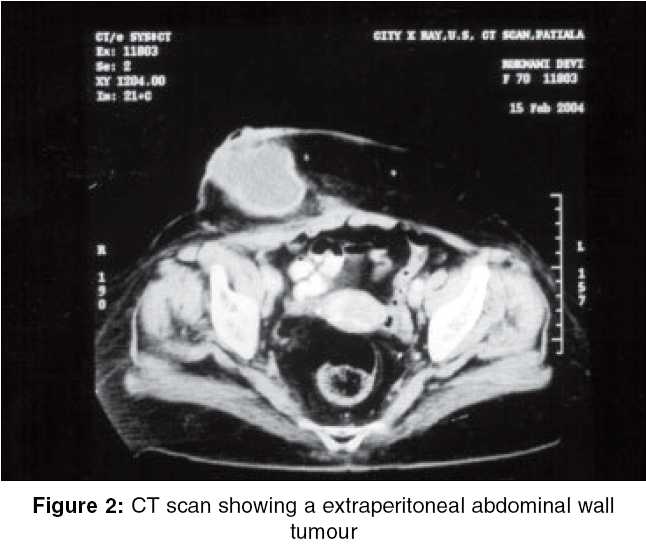
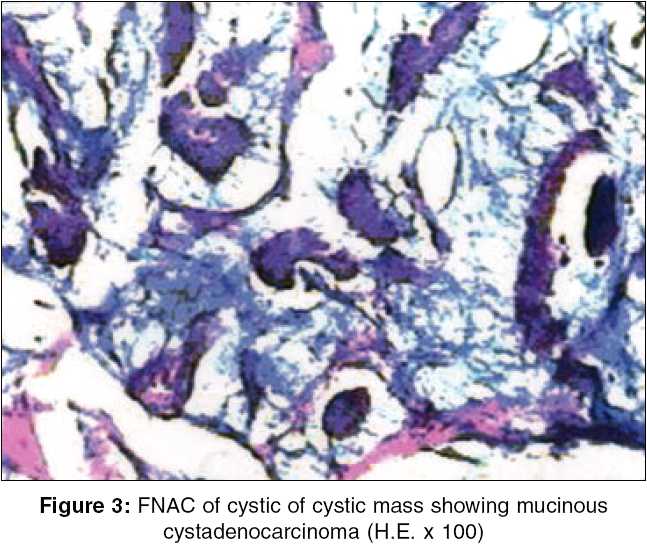
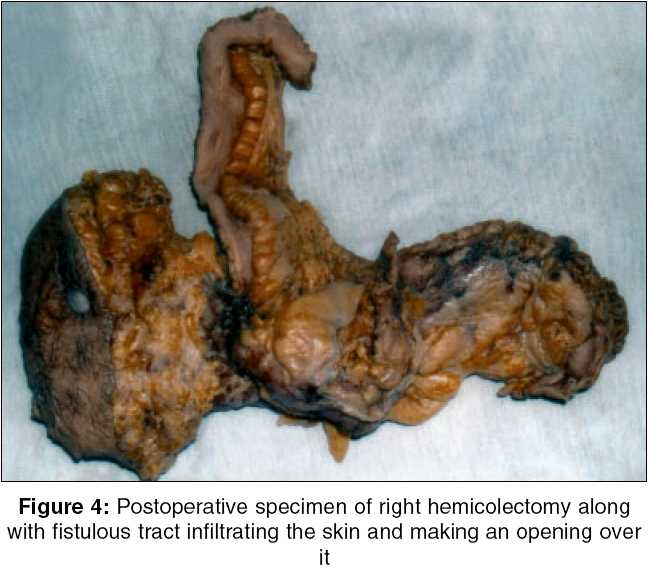
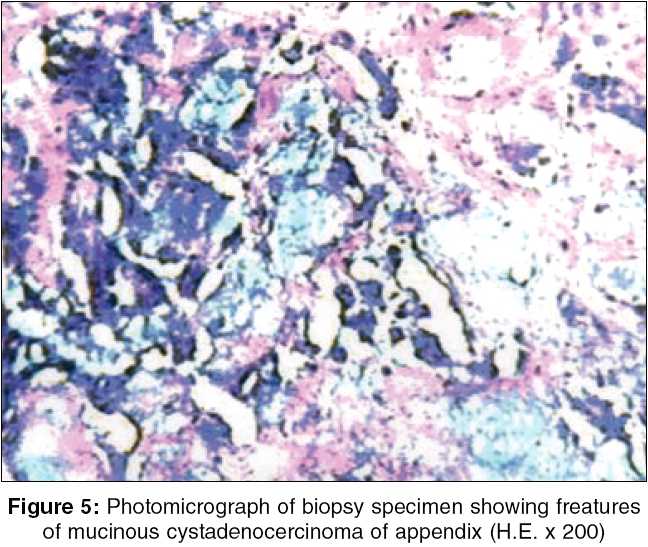
Indian Journal of Surgery, Vol. 67, No. 5, September-October, 2005, pp. 267-269 Case Reports Cystadenocarcinoma of appendix with cutaneous fistula - An unusual case presentation Grover AS, Mittal S, Singla P, Singh P, Kapoor W Department of General Surgery, Government Medical College and Rajindra Hospital, Patiala, Punjab Code Number: is05083 Abstract Cystadenocarcinoma of appendix is a rare tumour, usually presenting after middle age as acute appendicitis. It is seldom recognized during appendicectomy if localized to appendix. When it spreads, it presents as mucocele of appendix or pseudomyxoma peritonei. But very rarely it may present in an unusual manner like, bladder infiltration mimicking bladder cancer, caecocaecal intussusception, hydronephrosis, vaginal bleeding and extraperitoneal infiltration. We are presenting a case report of patient who presented to us as abdominal wall tumour with multiple sinuses. On exploration it turned out to be mucinous cystadenocarcinoma of appendix infiltrating extraperitoneally and presenting as abdominal wall tumour with cutaneous fistula. Keywords: Appendix, cystadenocarcinoma, right hemicolectomy Mucinous cystadenocarcinoma is a rare and second most common tumour of the appendix[1] usually presenting with intraperitoneal spread in the form of mucocele or pseudomyxoma peritonei or very rarely extraperitoneally with abdominal wall mass with cutaneous fistula (as in our case). We report a case of mucinous cystadenocarcinoma of appendix with most unusual presentation. Case presentation A 60-year-old female presented as an emergency with a large swelling on the right lower abdominal wall, which was gradually progressing for the last 6-7 months. Patient had no bowel or urinary complaints. She was menopausal and without any h/o bleeding or discharge per vaginum. Clinically there was an extraperitoneal, well-defined, nontender mass in right lumbar region, extending into right iliac fossa. The mass was 11 x 8 cm in size with cystic consistency and having two to three small openings, through which mucinous material was coming out [Figure - 1]. P/R examination was unremarkable. P/V examination revealed retroverted uterus with clear bilateral fornices. No tenderness or mass was palpable par vaginum. Blood chemistry was with in normal limits. Transvaginal ultrasound showed an extraperitoneal mass with clear bilateral adenexa. Computed tomography scan revealed a purely abdominal wall tumour without any intraperitoneal extension [Figure - 2]. There was no ascites and abdominal lymphadenopathy. Differential diagnosis of myxoid variant of liposarcoma or desmoid tumour was made. However, FNAC showed features suggestive of mucinous cystadenocarcinoma [Figure - 3]. Wide excision of the mass with some reconstructive procedure of abdominal wall defect was planned. On exploration, it was found that, the mass was going deep through a fistulous tract into the peritoneal cavity and taking its origin from the posterior caecal wall near the ileocaecal junction. Appendix was however not separately defined. Mesenteric lymph nodes were also present. There were no ascites and any evidence of metastasis in liver. Uterus and both ovaries were normal. Right hemicolectomy [Figure - 4] with omentectomy followed by ileotransverse anastmosis and mesh repair for abdominal wall defect was done. Postoperatively patient made uneventful recovery and discharged in satisfactory condition. Biopsy report came out to be mucinous cystadenocarcinoma of appendix [Figure - 5]. In the near follow up (after 2 months) patient was asymptomatic without any local or systemic complication [Figure - 6].Discussion Primary adenocarcinoma of appendix is a rare neoplasm of GIT and constitute about 0.5% of all the tumours of GI tract. There are four major histological subtypes - cystic, colonic, carcinoid and adenocarcinoids. Carcinoids are most common, constituting nearly 90% of all the primary tumours of appendix. Mucinous cystadenocarcinoma is the second most common type of appendicular tumour. Macroscopically they produce mucin filled cystic dilatation of the appendix indistinguishable from that associated with benign tumours. Diagnosis of malignancy is made from two features - invasion of appendicular wall and identification of epithelial cells in peritoneal mucous collections.[1] Spread of the neoplasm above the diaphragm or invasion of abdominal viscera is exceptional and lymphatic and hematogenous spread is also very rarely seen. Sometime this tumour may present with an unusual manner like polyploid infiltration of the abdominal wall, bladder infiltration mimicking bladder carcinoma, caecocaecal intussusception, reetroperitoneal abscess, hydronephrosis or vaginal bleeding. [2],[3],[4],[5] Carcinoma of appendix has always been a diagnostic dilemma.[6] Patient usually presents with features of appendicitis. Some time he or she may present with distension of abdomen due to pseudomyxoma peritonei and obstruction of the gut due to involvement of the colon. Even if the appendicectomy has been performed previously, there are chances of developing cystadenocarcinoma of appendicular stump. The possibility of carcinoma in appendicular stump, which increases in size, should be born in mind.[7] Rarely, appendicular carcinoma, instead of spreading intraperitoneally, metastasizes to extraperitoneal space as in our case. This is associated with relatively good prognosis by preventing the development of pseudomyxoma peritonei.[8] The poor prognosis of cystadenocarcinoma of the appendix supports an aggressive approach in treating the patients with this tumour. Surgery, i.e. right hemicolectomy is the primary treatment of cystadenocarcinoma of appendix. Most often, surgeon is faced with an intraoperative or postoperative diagnosis after appendicectomy, then second operation in form of right hemicolectomy should be done.[6] As pseudomyxoma peritonei usually arises from the ovary, followed by appendix, palliative oophrectomy is indicated for patients with ovarian metastasis because of the symptomatic nature of the metastasis. Surgical treatment must include right hemicolectomy, aggressive debulking (if tumour is unresectable), omentectomy, drainage of mucinous material and the excision of neighbouring compromised organs. The follow up thus must be lengthy consisting the possibility of the late recurrences.[6] In conclusion, right hemicolectomy is considered the treatment of choice in patients with cystadenocarcinoma of the appendix. Palliative oophorectomy is indicated for patients with ovarian metastasis. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05083f6.jpg] [is05083f1.jpg] [is05083f5.jpg] [is05083f4.jpg] [is05083f2.jpg] [is05083f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}