 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
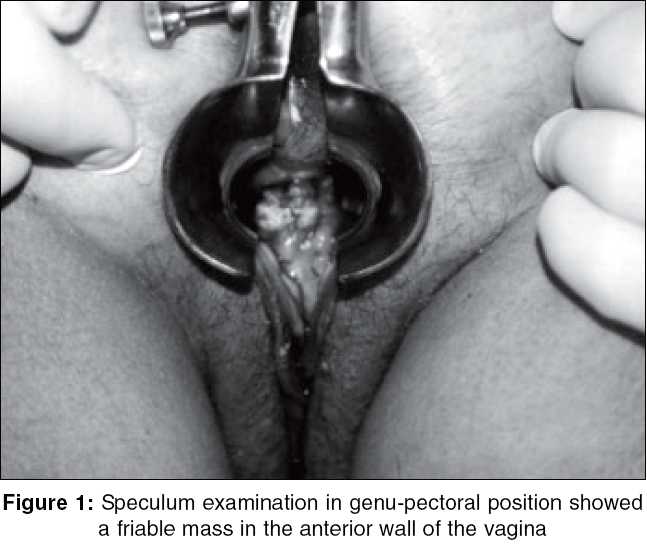
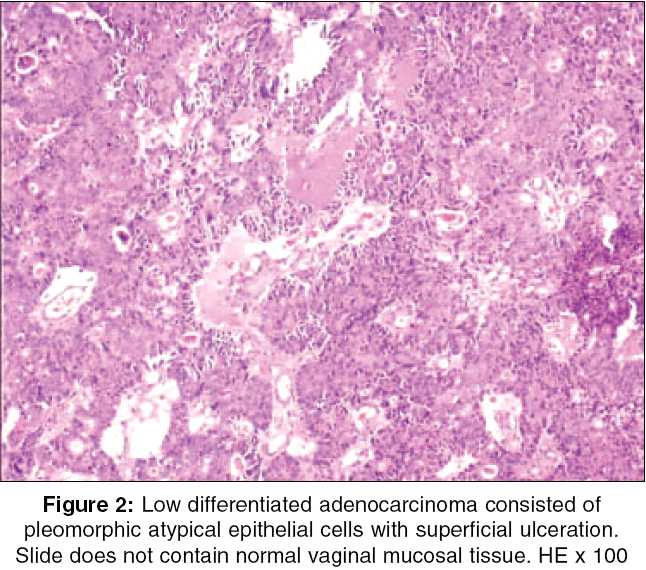
Indian Journal of Surgery, Vol. 67, No. 5, September-October, 2005, pp. 270-272 Case Reports True vaginal metastasis of rectal cancer Yagci G, Cetiner S, Dede M1, Gunhan O2 Departments of Surgery, 1Gynecology Obstetrics and 2Pathology, Gulhane Military Medical Academy, Etlik, Ankara, Turkey Code Number: is05084 Abstract Vaginal metastasis from colonic cancer is an extreme case and often indicates a poor prognosis. More frequently tumor cells from the colonic lesions spread out to vagina by direct contiguous way. We present a case of rectal carcinoma with true metastasis to the vagina that was discovered after an interval of 15 mounts when vaginal bleeding and discharge became evident. To our knowledge, there are only a few other papers in the English language previously documenting this phenomenon.Keywords: Adenocarcinoma, rectal neoplasms, vaginal neoplasms The first document in the literature regarding to vaginal metastasis of colorectal cancer was reported by Whitelaw[1] in 1956 when a vaginal lesion was found to be adenocarcinoma. Further investigation of the patient showed that primary tumor was originated from a mid-sigmoid tumor. In 1966, a series of four cases of remote vaginal metastases from colonic carcinoma was presented by Raider.[2] These lesions were found between 4 and 41 months after the initial colonic resection. In three of the four cases other sites of metastasis were also present with overall survival in these cases being less than 40 months. Since that time, however, there is only one other documented report of this interesting phenomenon was presented by Chagpar and Kanthan.[3] We report a rectal carcinoma case with true metastasis to the anterior wall of vagina. Case history Fifty-four-year-old woman presented to our clinic with left lower abdominal pain, rectal bleeding, weight loose, night sweets and dizziness. She had no previous history of medical illness. Physical examination revealed a soft abdomen with a slightly tenderness in left lower quadrant. Flexible recto-sigmoidoscopic examination showed a fragile tumor mass at 15 cm. And biopsy result of this lesion reported as adenocarcinoma with high mitotic activity and significant pleomorphism. Subsequent CT scan of the abdomen and ultrasound demonstrated a surface-seated liver nodule with diameters of 4.2-4.5 cm in segment 8 and a second small nodule in left lobe of liver with diameters of 2.8-2.4 cm both showing target sign. In the pelvic sections, there was thickening in the bowel wall beginning from rectosigmoid junction. Blood samples for tumor markers showed ten times fold in CA-19-9 and three times fold in CEA levels. Laparotomy with low anterior resection and tumorectomy of metastatic lesions in liver was performed. Postoperative period was uneventful and she was discharged without any complication. Pathology confirmed a poorly differentiated adenocarcinoma of the rectum invading the whole thickness of the bowel wall with surrounding fatty tissue. Tumor was 2.5 cm in diameter in the largest section invading a 6-cm long bowel segment. The specimen was tumor free in both resection borders. Tumor showed both lymphatic and vascular invasion and two out of ten lymph nodes were attacked by tumor cells. The patient was accepted as stage-IV rectum carcinoma and given six cycles of postoperative adjuvant chemotherapy by Oncology department with 5-FU plus calcium leucovorin periodically. During the follow-up period, she was admitted with 3 months intervals for the first year. Approximately 13 months after her first surgery, she came with bloody vaginal discharge and pelvic examination confirmed a 3 x 5 cm friable mass in the anterior wall of vagina [Figure - 1]. Bimanual pelvic examination revealed that vulva, cervix, uterus and bilateral adnexal structures are normal. Speculum examination showed a polypoid mass 2 x 3 cm in diameter on the anterior wall of vagina at fifth centimeter. Transabdominal pelvic ultrasound reported that the uterus was 34 x 37 x 41 cm in diameter, with homogeneous myometrium, indistinct endometrial echo pattern and bilateral adnexal areas were normal. Incisional biopsy was performed and reported as metastatic infiltration of poorly differentiated adenocarcinoma. The histological appearance of the tumor was similar to rectal carcinoma, which was diagnosed previously in the patient [Figure - 2]. The patient was then treated with intracavitary radiation and chemotherapy for the control of bleeding. Discussion Primary malignant vaginal tumors are rare and account only for approximately one percent of all malignant neoplasms of the female genital tract. Squamous cell carcinoma represents about 80% of malignant neoplasms primary to the vagina. Although primary neoplasms of the vagina are quite rare, secondary spread of malignant neoplasms to the vagina by direct extension or lymphatic or hematogenous metastasis is quite common.[4] Development of adenocarcinoma of the vagina in young women has been reported associated with maternal ingestion of diethylstilbestrol in utero with a rising incidence. These women should be examined regularly after menarche for prompt evaluation and treatment of precancerous lesions such as adenosis, cervical erosion or transverse ridges. Since most of these patients are young, a conservative treatment is recommended. Primary vaginal adenocarcinoma unrelated to intrauterine hormone exposure is very uncommon.[5],[6] Secondary vaginal adenocarcinoma represents 2.6% of all gynecological adenocarcinomas while 92.5% of apical lesions were metastasized from the upper genital tract, and 90.0% of the posterior lesions were from the gastrointestinal tract. About two-thirds of recurrences or metastases were reported after removal of primary lesions, and 80.8% occurred within first 3 years.[7] Fu and Reagan found that only 58 (16%) of 355 invasive carcinomas involving the vagina represented primary neoplasms. Spread from primary carcinoma of the cervix was most common (32%), followed by endometrium (18%), colon and rectum (9%) ovary (6%), vulva (6%), and urinary tract (4%). Even among the squamous carcinomas found in the vagina, only a minority prove to be primary to this side. About 75% are secondary, arising in either cervix (79%) or vulva (14%). Generally the vagina is a site for metastases from other areas of the female genitourinary tract.[8] Other miscellaneous tumors that have been found to have vaginal metastases include adenocarcinoma of pancreas, trophoblastic neoplasms, and tumors of the urinary tract. [9],[10],[11],[12] When direct contiguous spread is not the case, it is speculated that remote vaginal metastasis may occur either through lymphatic or hematogenous routes. Lymphatics from the sigmoid may carry metastasis to the iliac and hypogastric nodes where there could be retrograde spread to the periurethral area and anterior vaginal wall. Alternatively venous channels may allow the tumor emboli to pass from the colon to the ovarian plexus or parametrial veins and then on to the vaginal veins. Disseminated metastatic disease is frequently present in patients with vaginal metastases and the prognosis is extremely poor in these patients. In three of the four patients reported by Raider, there was evidence of widespread metastatic disease. In these patients overall survival ranged from 10 to 39 months after the diagnosis of vaginal metastasis. The one case that had no other metastatic involvement, however, remained alive and well 48 months after the vaginal lesion was treated with intracavitary radiation.[2] Although it is frequently associated with primary vaginal tumors, vaginal bleeding or discharge might be the first clinical manifestations of an occult carcinoma or clinical signs of a widespread metastatic disease. We present a case of rectal carcinoma with true metastasis to the vagina that was discovered after an interval of 15 mounts when vaginal bleeding and discharge became evident. Intracavitary radiation and chemotherapy was effective for the control of bleeding whereas angiographic embolization may be emerging as a successful procedure to control the severe hemorrhage. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05084f1.jpg] [is05084f2.jpg] |
| |||||||||

{kind=link}
{kind=link}