 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
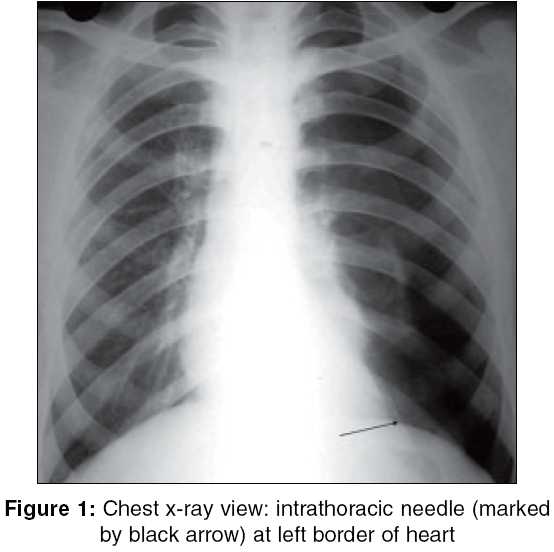
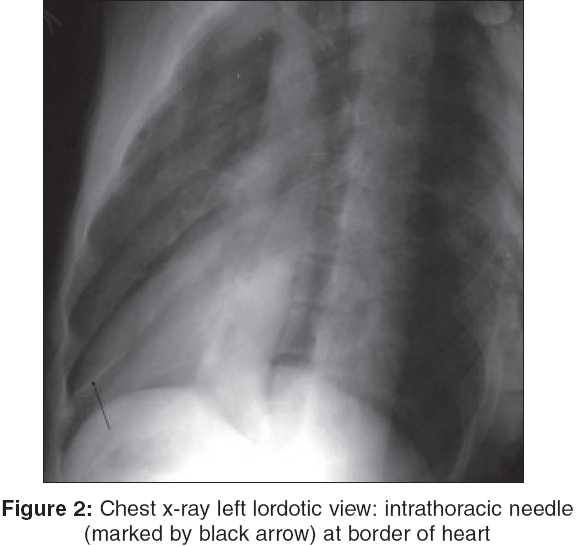
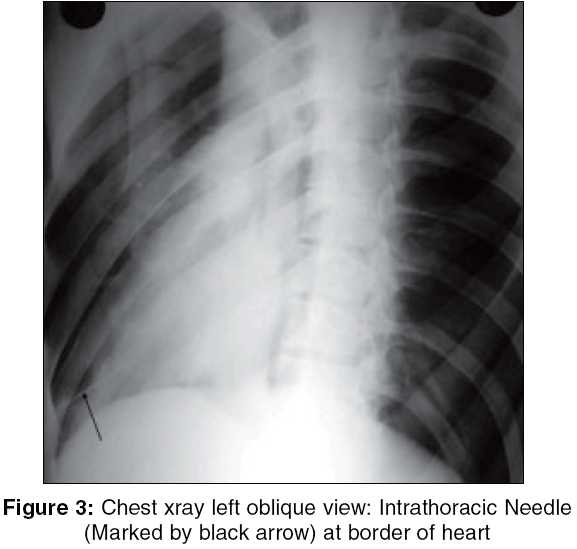
Indian Journal of Surgery, Vol. 67, No. 5, September-October, 2005, pp. 276-277 Images in Surgery Intrathoracic foreign body: Straight sewing needle in pericardial cavity Darbari A, Chandra G, Pandey S, Tandon S Department of C.T.V.S., K. G. M. University, Lucknow, Uttar Prdesh Code Number: is05086 A 25 years male of average built, a tailor by profession, was admitted in our institute on 09.10.2004. A straight sewing needle had pierced his chest wall just below left nipple, 10 days back. This needle was fixed in his shirt′s pocket. Blind surgical exploration tried, but failed. Patient was having no dyspnoea, but chest X-ray PA, left lateral and lordotic oblique view showed left pneumothorax with needle inside thoracic cavity at left border of heart.[Figure - 1][Figure - 2][Figure - 3] Video assisted thoracoscopy tried on 11.10.2004 under general anaesthesia, but we were unable to find the needle. In the same sitting, open exploration by left anterior thoracotomy done. A straight sewing needle found, which was totally inside thoracic cavity and embeded in pericardial fat at lower left border of heart near apex. It was freely moving with heart activities, but on opening pericardium, no injury to inside structures of heart was found. Sewing needle taken out. Left lung was normal. Postoperative patient′s recovery was uneventful. Intrathoracic Foreign bodies specially inside heart or mediastinum are rare. Generally they occur during war, penetrating trauma, misplaced central venous cathater [1] and intrathoracic migration of Kirschner pins used for the treatment of sternoclavicular joint dislocation.[2] If it is radio opaque, the initial localization by X-ray or CT scan is noteworthy, because they may embolize later. Removal is warranted for this risk. Get′man VG. [3] analyzed the use of thoracoscopy in patients with radiopaque and radiolucent foreign bodies in the thoracic cavity. Thoracoscopy made it possible to detect not only foreign bodies of different character, but also the damages caused by them to the viscera, and the complications. Foreign bodies were removed during thoracoscopy in two-thirds of cases. For remaining one-third cases, open exploration had to be done[4]. References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05086f3.jpg] [is05086f1.jpg] [is05086f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}