 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
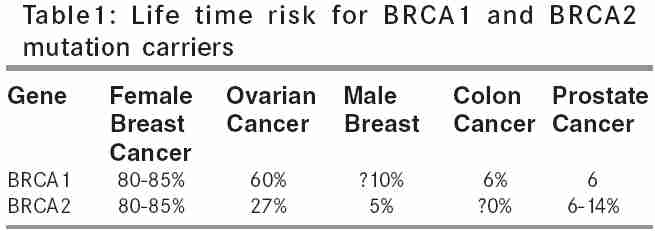
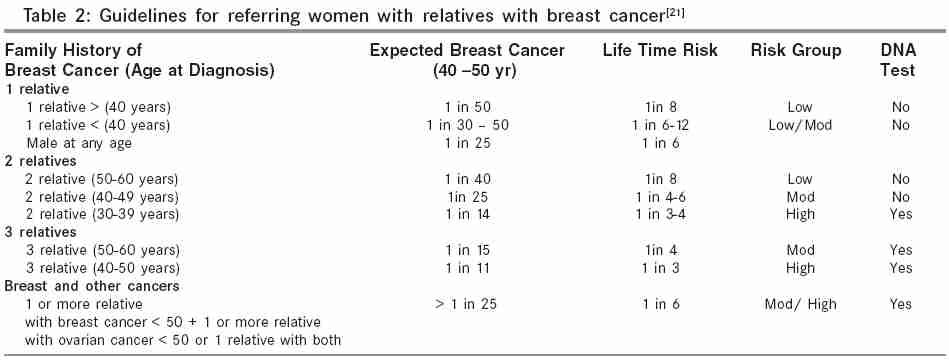
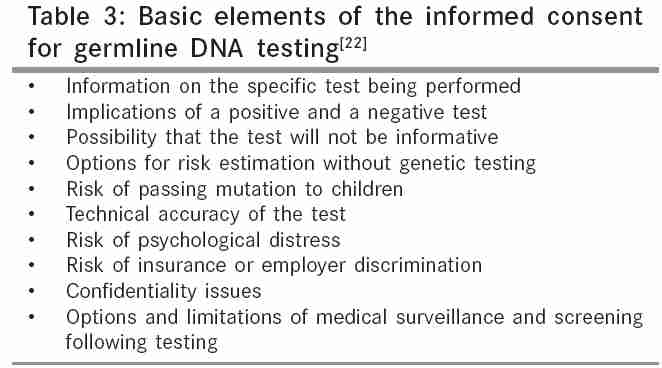
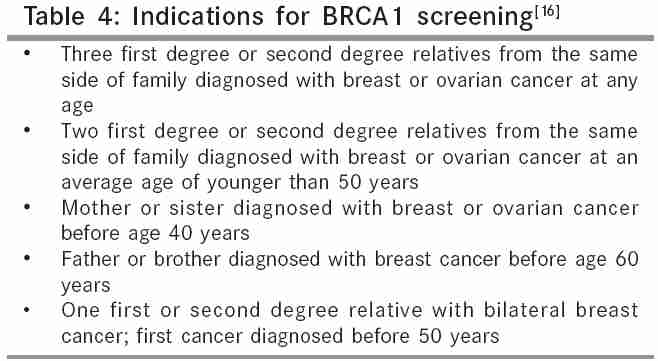
Indian Journal of Surgery, Vol. 67, No. 6, November-December, 2005, pp. 297-301 Review Article Familial breast cancer: Genetics and counseling Thakur S, Phadke SR Department of Medical Genetics, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India Code Number: is05091 Abstract Hereditary breast cancer (HBC) accounts for 5-10% of all breast cancer cases. A family history of breast cancer has long been ecognized as a significant risk factor for breast cancer. Mutations in BRCA1 and BRCA2 account for about 40% of the cases. So, overall they constitute less than 5% of all of the breast cancer cases. With increasing awareness women with family history often overestimate their personal risk for breast cancer and may view themselves as candidate for genetic testing. Identification of high risk cases needing genetic counseling and DNA testing is needed. In this article we have reviewed the genetics of breast cancer and the genetic counseling protocol to meet the needs of women with family history of breast cancer.Keywords: Familial breast cancer, BRCA1, BRCA2, genetic counseling Introduction Breast cancer is the commonest malignancy of women in the world. It accounts for about 18% of female cancer cases.[1] The overall incidence of cancer in India is 36.2/100,000 population with marked variation in the different regions of the country. In males cancer of lung, stomach, cancer of oesophagus are the commonest sites of cancer. In females cancer breast is the commonest neoplasm in most of the areas except Chennai where cancer of cervix is the cancer.[2] Various risk factors implicated are age at menarche, age at first live born child, breast feeding and family history of breast or ovarian cancer. Of all these family history is the strongest known epidemiological factor. Most of the breast cancer cases are sporadic, only 5-10% are hereditary and are due to germline mutations in susceptibility genes.[3],[4] Inheritance is as autosomal dominant pattern Two major genes associated with the susceptibility to breast and ovarian cancer are BRCA1 and BRCA2. BRCA1 and BRCA2 mutations are found in 40% of families with evidence of inherited susceptibility to the breast and ovarian cancer.[4] Other genes in the breast cancer susceptibility are CHECK2 (5%), TP53 (< 1%), ATM gene and PTEN gene.[5],[6] In addition unidentified number of susceptibility genes and environmental factors are likely to play an important role in the remaining 50% of cases. Genes associated with hereditary breast cancer BRCA1 and BRCA2 account for about 40% of families with evidence of inherited susceptibility to breast cancer. Life time risk for the mutation carriers of BRCA genes are 60-85% for breast cancer and that of ovarian cancer 15-40%.[7],[8] Life time risk for developing various cancers in the mutation carriers of BRCA genes are shown in [Table - 1]. BRCA1 and BRCA2 are tumor suppressor genes. The individuals with inherited susceptibility to these genes carry an inactivating mutation in one copy of the gene in the germ line. That is the mutation is present in all cells of the body. A single event rendering the second copy of the gene nonfunctional initiates malignancy. Germline mutation in the BRCA1 and BRCA2 are transmitted in autosomal dominant manner, i.e. the offspring of the mutation carrier have a 50% chance of inheriting the mutation. Population genetics of BRCA1 and BRCA2 The proportion of high risk families with breast or ovarian cancer attributable to BRCA1 mutation varies widely among populations. BRCA1 mutation are most common in Russia accounts for 79% of hereditary cancer breast while the prevalence is 47% in Israel and 27% in Italy.[9] Between 20-25% of high risk families in Britain, France, Scandinavia and Hungary have BRCA1 mutation. In Japan the incidence of BRCA1 mutation is 10% and in Iceland 9%. Various Indian studies have reported BRCA mutations in 9-25% of familial breast cancer cases. [10],[11],[12],[13],[14] In most populations 6-10% of patients with breast cancer have mutation in BRCA gene irrespective of their family history. In most population frequency of BRCA1 mutation is higher compared to BRCA2 by a factor of 1.5-2 except in Iceland where the frequency of BRCA2 is higher (64%).[3] In Israel 24% of hereditary breast and ovarian cancer families are due to BRCA2 mutation. In the United States and Canadian families the percentages are 25% and 16% respectively. Lower prevalence of BRCA2 mutation could be due to fewer mutations, lower penetrance and/or to later age of onset in the BRCA2 carrier. In families with male breast cancer BRCA2 mutation are more common than BRCA1. In at least 50-60% of the families no mutations in both BRCA1 and BRCA2 have been detected. Structure and function of BRCA1 BRCA1 is mapped to chromosome 17q21.[15] It is a large gene and spans over 100 Kb. It has 24 exons of which only 22 are coding. Out of which exon 11 is very large. The gene encodes a protein of 1863 amino acids (220kDa). It contains a RING finger domain near the N- terminus and an acidic carboxy terminal domain characteristic of many trascription factors. RING finger domain is critical for the function of BRCA1. It serves as an interface for recognition of DNA or protein- protein interaction. The BARD1 gene located on chromosome 2q33-34 interacts with RING finger domain and is involved in tumor suppression and mutations in the RING finger domain hence result in defective tumor suppression. BRCT domain is present at C- terminus. This domain is involved in cell cycle regulation in response to DNA damage. Mutations in BRCA1 gene More than 600 different mutations have been described in BRCA1 gene.[16] They are scattered throughout the coding region of the gene and more than 50% of them have been described only once. 95% of mutations result in the truncation of protein. 70% of the mutations are frame shifts, 20% are nonsense. Splice site and missense mutations constitute about 5% each. The three common mutations are 1. Mutation in the RING finger domain 185 delAG - 12% Structure of BRCA2 BRCA2 is the second breast cancer susceptibility gene that is mapped to chromosome 13q12-q13.[17] BRCA2 is a large gene almost twice as large as BRCA1. It is composed of 27 exons and encodes a protein of 3418 amino acids. The type of mutations is frameshift mutation (68%), nonsense (12%), splice sites (7%) and missense (13%). The types of mutations vary within different population. The mutations can be classified as recurring or unique. Unique mutations are confined to a population. The incidence of mutation carriers is very high in Ashkenazi Jews (1 in 40 to 1 in 50). The three common founder mutations in Ashkenazi Jews are BRCA1 185delAG, 5382insC and BRCA2 6174delT. In Iceland founder mutation is BRCA2 999del5. In Russia common alleles of BRCA1 are 532insC and 4153delA. 532insC mutation is also the most common allele among Europeans whereas 4153delA has not been observed outside Russia so far. Many European BRCA1 and BRCA2 mutation has been observed in United States and Canada reflecting European migration to North America. Techniques of mutation detection 1. Protein truncation test Protein truncation test is done for exon 11 of BRCA1 and exon 11 and exon 12 of BRCA2. Protein truncation test detects premature stop codons in a single reaction by amplifying DNA fragments of the coding region. Single stranded conformational polymorphism (SSCP) is used for the analysis of exon 2-10 and exon 12-24 of BRCA1 and exon 2-10 and exon 12-27 of BRCA2. Here the conformational change in the DNA due to point mutation affects the mobility in the gel. All the variants identified by both methods are verified by sequencing. The large number of mutations and specialized tests required for identification of each makes detection of mutation tedious and costly. Other breast cancer genes TP53 gene ATM gene PTEN gene Genetic counseling for women with family history of breast cancer The steps involved in advising women with breast cancer 1. Correct diagnosis of cancer and its hereditary predisposition Correct diagnosis of cancer and determination of its hereditary predisposition is cornerstone of the meaningful genetic counseling. This is achieved by constructing a three generation pedigree and enquiring about the family history of cancer in first degree as well as distant relatives on both paternal and maternal side. Cancer of all anatomic sites in addition to breast cancer must be addressed. The pedigree should document the primary tumor site, age of onset, presence of bilateral or multiple primary tumors, ethnicity and age of affected relatives. Pedigree development is a dynamic process and so new changes over time must be added. Risk assessment Family history of breast cancer is usually taken as strongest epidemiological factor. The risk of breast cancer depends upon the age of onset in the proband and the number of relatives. Life time risk of breast cancer in general population is 9% and the patients are divided according to the risk in three groups[21] a. Low risk <2 times population life time risk The risk calculation based on family history, age of onset and presence of male breast and ovarian cancer. The guideline for referral and mammography in the women with one, two or three relatives affected with breast cancer is shown in the [Table - 2]. The table shows that women with high risk of breast cancer are · Two relatives diagnosed with breast cancer at age 30-39 Possible options for high risk women The natural history of breast cancer mandates that high risk women receive special attention. Education is initiated in midteens. This involves a description of the natural history of HBC. At age 18 years they are taught self breast examination. They are then told in detail about pros and cons of genetic testing. Mutation detection test of at risk women clears the uncertainties and identifies mutation carriers who are at high risk of cancer breast. Absence of mutation makes intensive surveillance from early age unnecessary. Identification of mutation in the affected relative with breast cancer is the prerequisite before offering mutation test to the at risk family members. Pretest genetic counseling is mandatory before DNA testing. Basic elements of informed consent for germline DNA testing are given in [Table - 3].[22] All matters including implications of a positive test, implications of a negative test, and limitations of the testing, the options for risk estimation without genetic testing, the risk of passing a mutation to children, the technical accuracy of the test, the cost of testing, the risk of psychological distress, the risk of discrimination and options and limitation of medical surveillance and screening following testing should be clearly discussed. The disclosure of BRCA1/2 testing is usually done face to face and the various methods of reducing risk in mutation carriers are discussed. The possible options of early diagnosis and management of germ line BRCA1 and BRCA2 carriers are given.[23] Cancer surveillance should begun at early age because they are at risk of cancer at an early age. Breast cancer surveillance is done by self breast examination (18 years), annual clinical examination and mammography annually or semiannually beginning at the age of 25 years. Prophylactic mastectomy can be offered as mastectomy has been shown to cause 90% reduction in incidence of cancer in mutation carriers and 80% reduction in the cancer related deaths.[24] Bilateral prophylactic oophorectomy reduces the risk of ovarian cancer by 95% and the risk of breast cancer by 53%. Bilateral prophylactic oophorectomy should be done as soon as the child bearing is completed. [25] Though highly effective prophylactic surgery involves complex psychosocial issues and the option may not be acceptable to many. Chemoprevention of breast cancer using Tamoxifen can be tried. Predictive genetic testing Indications for predictive genetic testing are given in [Table - 4].[16] Mutation detection does not alter the management of cancer in such women. As mutation in BRCA1 and BRCA2 account for 5-6% of cases of breast and ovarian cancer cases, DNA test is not necessary for each case of breast and ovarian cancer. DNA test is considered necessary when the possibility that the particular family in concern is likely to have familial breast cancer is more than 10%. Mutation detection does not alter the management of cancer in such women but it is necessary for providing DNA test to at risk relatives. If a mutation is not identified in the affected member of the family; DNA test can not be offered to the at risk members of the family. In 30-40% of cases of hereditary breast cancer the predisposing gene is unknown. Advantages of predictive testing are 1. Increased knowledge about cancer risk and Disadvantages of such testing are Conclusions Hereditary breast cancer account for about 5-10% of cases of breast cancer. The two most important genes in familial cancer are BRCA1 and BRCA2 which together account for about 40% of familial breast cancers. The DNA test gives complete reassurance and removes the option of intensive surveillance programme and prophylactic surgery. But it is only possible when the mutation in the affected family member is identified. Mutation detection tests are costly, tedious and not available easily. Mutation detection confirms the inherited nature of the cancer but if mutation is not detected it does not rule out the possibility of genetic susceptibility to breast cancer The genetic testing should be only done when there is strong contribution of hereditary component as suggested by family history. The test should not be done without availability of adequate pretest and post test counseling. The preventive options for mutation carriers are surveillance for early detection by mammography, prophylactic mastectomy and prophylactic oophorectomy. Women with high risk in whom mutation is not identified or can not be tested are candidates for same preventive options as those for BRCA1 and BRCA2 carriers for early diagnosis and management.References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05091t3.jpg] [is05091t1.jpg] [is05091t5.jpg] [is05091t4.jpg] [is05091t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}