 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
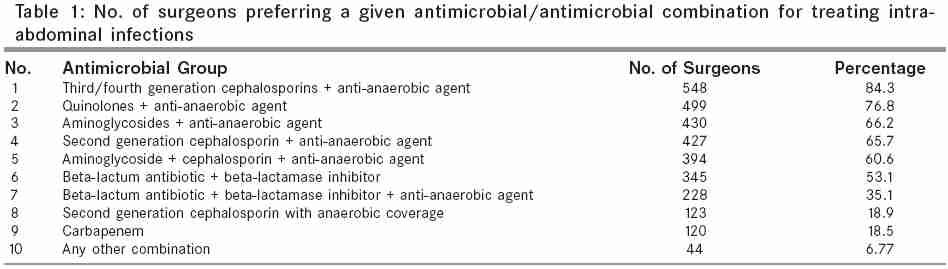
Indian Journal of Surgery, Vol. 67, No. 6, November-December, 2005, pp. 308-315 Original Article Patterns of antimicrobial use by surgeons in India Kulkarni RA, Kochhar* PH, Dargude VA, Rajadhyakshya* SS, Thatte UM Department of Clinical Pharmacology, TN Medical College and BYL Nair Ch. Hospital, Mumbai 400008, India.*Pfizer India Ltd. Code Number: is05093 Abstract Background: In spite of several available guidelines for the appropriate use of antimicrobials in perioperative patients, the fear of high morbidity and mortality associated with Intra-abdominal infections and Surgical Site Infections has led to misuse of antimicrobials in the perioperative period.Aims: This study was conducted to ascertain the antibiotic prescribing patterns of surgeons for treatment of intraabdominal infections and surgical prophylaxis and specifically assess the prescribing patterns of surgeons at Institutions with a Hospital Infection Control Committee (HICC). Setting and Design: Questionnaire survey at ASICON 2003. Materials and Methods: A survey was conducted among surgeons from all over India attending the conference to ascertain the prevalent prescribing trends for treatment of intraabdominal infections and surgical prophylaxis and the average duration of treatment. Surgeons were also requested to indicate the presence of a HICC. Results: 650 surgeons of the 700 asked, filled in the questionnaire legibly. It was observed that third/fourth generation cephalosporin plus an anti-anaerobic agent were preferred for treating intra-abdominal infections (84%) for an average duration of 6.38 + 2.2 days. For surgical prophylaxis, we found that 55% of the surgeons prescribed a single antibiotic for clean surgeries. A combination of two or three antimicrobial agents was preferred in clean contaminated (42.3%) and dirty (46.9%) surgeries respectively. Third generation cephalosporins were the commonly prescribed antibiotics (80%) for all surgeries. However, antibiotics were prescribed for durations longer than recommended in standard guidelines. Although 260 surgeons stated that their Institution had an HICC, this had no major impact on the prescribing trends. Conclusion: There is an urgent need to promote rational antimicrobial prescribing among surgeons and to formulate National guidelines for appropriate use of antibiotics in surgical practice. Keywords: Antibiotic prescribing, intra-abdominal infections, surgical prophylaxis, clean surgeries, clean contaminated surgeries, dirty surgeries INTRODUCTION Antimicrobial drug resistance is a growing problem worldwide.[1],[2] The widespread and often inappropriate use of broad spectrum antimicrobial agents is recognized as a significant contributing factor to the development and spread of bacterial resistance.[3] However, despite these well-publicized concerns, the inappropriate use of antimicrobials still persists.[4],[5] The consequences of development of drug resistance include higher mortality and greater morbidity, longer hospitalization periods and greater expense.[6] The Indian scenario too, is dismal with regard to antimicrobial prescribing and publications have documented the irrational prescribing patterns in various settings.[7],[8] The fear of morbidity and mortality associated with intra-abdominal infections and Surgical Site Infections (SSI) has lead to high usage of antimicrobials in the peri-operative period. Despite recommendations and guidelines formulated by various surgical committees regarding appropriate use of antimicrobials,[9],[10] these are rarely implemented in practice. Also, not many institutions have an active Hospital Infection Control Committee (HICC) or established Institutional guidelines to streamline the antimicrobial prescribing practices. Hence various forms of inappropriate prescribing often remain unnoticed. Assessment of current antibiotic prescribing patterns is an important step towards promoting appropriate use of antimicrobial agents. The present survey was conducted to gain insight into the prevalent antimicrobial prescribing trends among surgeons all over India for treating intra-abdominal infections as well as to determine the choice of antimicrobials for surgical prophylaxis. Also, an attempt was made to assess the number of Institutions having an established Hospital Infection Control Committee (HICC) and the prescribing practices of the surgeons in these Institutions. PATIENTS AND METHODS A survey regarding antimicrobial usage was conducted among surgeons attending the Association of Surgeons of India Conference (ASICON) in December 2003. The surgeons were requested to complete a questionnaire that posed the following questions. 1. The choice of antimicrobial(s) for the treatment of intra-abdominal infections. The surgeons could make a choice of more than one antimicrobial/ antimicrobial combination. The surgeons were also requested to provide information regarding the presence of a Hospital or Institutional Infection Control Committee. The data was analysed and the results depicted as percentages. RESULTS Surgeons from all over India attending the ASICON 2003 conference were contacted and requested to fill the questionnaire. Of the 700 surgeons that responded, 650 questionnaires were legible and were used for analysis. Profile of responding surgeons Out of the 650 responders, 254 surgeons were practicing in private hospitals and 247 were employed in public hospitals. The Institutional profile of the remaining surgeons is unknown. They were well represented from all parts of the country i.e. north, south, east, west & central India. There was a larger representation by surgeons from the non-metro cities (84.6%) than from the metro cities (15.4%). Choice of anti-microbial agents for treating intra-abdominal infections The questionnaire inquiring about preferred antimicrobials for treating intra-abdominal infections permitted surgeons to list more than one choice of antimicrobials or antimicrobial combination. [Table - 1] summarizes the antibiotic combinations in the descending order of frequency of preference. The analysis revealed that a third/fourth generation cephalosporin along with an anti- anaerobic agent was the most preferred antimicrobial combination for treating intra-abdominal infections (84%). This was followed by a quinolone or an aminoglycoside in combination with an anti- anaerobic agent. A triple drug combination (aminoglycoside + cephalosporin + anti-anerobe) was preferred by over 60% surgeons. Some surgeons (18%) used a single antimicrobial with broad coverage. The duration of treatment ranged from a minimum of 1 day to a maximum of up to 20 days. The average duration of the antimicrobial therapy was 6.38 + 2.2 days. Peri-operative surgical prophylaxis Of 650 surgeons, only 38 (5.85%) and 2 (0.31%) surgeons preferred not to use any antimicrobial prophylaxis for clean and clean contaminated surgeries respectively. Data on 6 surgeons regarding antimicrobial prophylaxis in dirty surgery was not available A single antimicrobial agent was preferred by a large percentage of surgeons (54.9%) in clean surgeries, whereas combination of two and three antimicrobial agents was preferred in case of clean contaminated (42.3%) and dirty (46.9%) surgeries respectively. Some surgeons (1.4%) used a combination of four antimicrobials in dirty surgeries [Table - 2]. Choice of antimicrobials in peri-operative prophylaxis Cephalosporins were the most commonly prescribed antimicrobials (39%) across all surgery groups viz . clean, contaminated and dirty surgeries [Figure - 1]. Penicillins and quinolones were most commonly used in clean surgeries whereas anti-anaerobic agents and aminoglycosides were prescribed more frequently in cases of clean contaminated and dirty surgeries. Among the cephalosporins, more than 80% of the surgeons preferred third generation cephalosporins, particularly ceftriaxone and cefotaxime, for all types of surgeries. Ceftriaxone was the preferred choice for clean (32.4%) and dirty (25.19%) surgeries while cefotaxime was most often used for clean contaminated surgeries (33.39%). Fourth generation cephalosporins such as Cefepime & Cefpirome were preferred in case of dirty surgeries. In case of quinolones, Ciprofloxacin (38% in dirty surgeries to 67% in clean surgeries) was the most commonly used antimicrobial agent in all types of surgeries. Ampicillin (17% in dirty surgeries to 37% in clean surgeries) was the preferred antibiotic in case of Penicillins in all types of surgeries. In case of combinations of two antimicrobial agents, cephalosporins in combination with an anti-anaerobic agent was the preferred two drug combination for all types of surgeries (17% in clean surgeries to 40% in dirty surgeries) followed by Cephalosporins in combination with Aminoglycosides (17% in clean surgeries to 30% in dirty surgeries) In case of combinations of three antimicrobial agents , c ephalosporins in combination with an aminoglycoside and an anti-anaerobic agent was the preferred three drug combination in all types of surgeries (34% in clean surgeries to 75% in dirty surgeries). Penicillins (52%) or Quinolones (52%) were the alternative choices instead of Cephalosporins mainly in dirty surgeries. Further analysis of the preferences of surgeons with respect to the type of surgery showed that 3rd or 4th generation cephalosporins or a combination of 2nd 3rd or 4th generation Cephalosporins plus an aminoglycoside plus an anti-anerobic agent were the preferred choices in case of all three types of surgeries. Comparison of the choice of antibiotic and the duration of use by the surgeons with the available guidelines for antimicrobial prophylaxis showed that 51 (8%), 39 (6%) and 4 (0.6%) surgeons were prescribing as per the guidelines in clean, clean contaminated and dirty surgeries respectively. [Table - 3][Table - 4][Table - 5] Presence of Hospital Infection Control Committee (HICC) 260 (40%) surgeons stated that their hospital/Institution had a Hospital Infection Control Committee (HICC). Of these, 102 (39.23%) respondents were affiliated to private institutions while 94 (36.2%) were attached to public hospitals. 64 (24.6%) surgeons affirmed the presence of HICC at their hospital but the Institutional details were not available. Of these 260 surgeons, 6% did not use antimicrobials while 59.62% used a single antimicrobial agent in clean surgeries. 43% used two antimicrobial agents and 45% used three antimicrobial agents in clean contaminated surgeries and dirty surgeries respectively [Table - 6].Further analysis of the preferences of these surgeons with respect to the type of surgery showed that cephalosporins, penicillins or a combination of pencillins plus an aminoglycoside plus an anti-anerobic agent were the preferred choices in case of clean surgeries, while 3rd or 4th generation cephalosporins or a combination of 2nd, 3rd or 4th generation Cephalosporins plus an aminoglycoside plus an anti-anerobic agent were preferred in case of clean contaminated and dirty of surgeries. Comparison of the choice of antibiotic and the duration of use by the surgeons with the available guidelines for antimicrobial prophylaxis showed that 22 (8.5%) and 11 (4.2%) surgeons were prescribing as per the guidelines in clean and clean contaminated surgeries respectively while none of the surgeons were prescribing as per the guidelines in case of dirty surgeries. [Table - 7][Table - 8][Table - 9] DISCUSSION A great amount of concern has been voiced in the past two decades regarding the widespread use of antimicrobials, leading to emergence of multiple drug-resistant organisms.[11] Almost 30% to 50% of the use of these agents is unnecessary, especially for prolonged periods.[12] Considerable efforts have been made in recent years to educate physicians and the public about the importance of minimizing the unnecessary use of antimicrobials. [13],[14],[15],[16] This survey provided information regarding the antimicrobial prescribing practices of surgeons in India for treating intra-abdominal infections as well as for surgical prophylaxis. Intra-abdominal infections are commonly polymicrobial and correlate directly with the unique endogenous microflora at various levels of the gastrointestinal tract.[17] A perplexing problem is whether to provide empirical anti-infective therapy for the wide range of microorganisms that are commonly encountered. Empirical therapy may not always be effective and may promote antimicrobial resistance.[18] The Surgical Infection Society (SIS) Guidelines state that antimicrobial regimens for intra-abdominal infections should cover common aerobic and anaerobic enteric flora.[9] Single agents like ampicillin/sulbactum or cefoxitin are effective. Combination regimens include third/ fourth generation cephalosporin plus an anti-anaerobe (clindamycin or metronidazole), aminoglycoside plus an antianaerobe, quinolone plus metronidazole etc. However, no regimen has been found to be superior to the other.[9],[19] In keeping with these guidelines, our survey revealed that a combination of third/ fourth generation cephalosporin and an anti-anaerobic agent was the most popular regimen, prescribed by nearly 85% of the respondents. However it was disturbing to note that more than 60% surgeons used combinations of three drugs (cephalosporin + aminoglycoside + anti-anaerobe). Routine addition of an aminoglycoside to other agents having broad-spectrum gram-negative coverage, such as 3rd/4th generation cephalosporins has been shown to provide no additional benefit.[9] There is growing consensus that shorter, rather than prolonged, courses of therapy are appropriate for most patients with intra-abdominal infections. This minimizes the patient exposure to toxic and expensive agents as well as prevents emergence of resistant organisms. SIS guidelines recommend 5-7 days of therapy.[9] In our survey, the average duration of antimicrobial therapy was 6.38 + 2.2 days, which was conforming to standard guidelines. There have been many reports and guidelines on the prevention of surgical site infections (SSI) and use of antimicrobial prophylaxis in surgeries.[9],[20],[21] Scottish Intercollegiate Guidelines Network (SIGN) guidelines advocate that antimicrobial prophylaxis should depend upon the patient's risk of SSI, the potential gravity of the consequences of SSI and the effectiveness of prophylaxis.[22] It is recommended that prophylaxis should be administered immediately before, or during a procedure and should provide coverage against common pathogens. In event of delayed or prolonged surgery, a second dose is advisable if an antimicrobial drug with a short half-life is used. Guidelines mention that prophylactic antimicrobials should certainly be discontinued within 24 hours of the operative procedure.[9],[19],[20],[22] Prolonged post-operative administration is unnecessary and harmful. Perhaps the biggest controversy in surgical prophylaxis relates to the use of antimicrobials in clean surgery.[23] Whether benefits outweigh the risks, has been questioned for "clean," low risk procedures like hernia repair and skin surgery, although there is data to show that antibiotic prophylaxis is beneficial when the risk of infection is high (e.g. patient is very sick or requires a long complicated hernia operation).[23] It is widely agreed that antimicrobial prophylaxis is beneficial in operations entailing entry of the gastrointestinal tract, due to consequent exposure of the surgical wound to endogenous intestinal bacteria.[20],[22] In clean contaminated and dirty surgeries, usually a combination of two or three antimicrobial agents are suitable for surgical prophylaxis. In our study too, about 42% of the surgeons used a combination of 2 antibiotics in case of clean contaminated surgeries and 45% used 3 antibiotics in case of dirty surgeries. Less than 2% of the surgeons prescribed 4 antibiotic groups prophylactically. Also, as seen in the case of clean surgeries, antibiotics were being given for durations longer than recommended in standard guidelines with up to nearly three weeks in clean contaminated and dirty cases. Only 6% and less than 1% of the surgeons stopped antibiotics after 24 hours in clean contaminated and dirty surgeries respectively. The use of cephalosporins in our study was similar to that reported in literature.[24],[25],[26] Cephalosporins are recommended for surgical prophylaxis due to their good safety profile, excellent antimicrobial activity broad spectrum and efficacy against common pathogens. Cefazolin (first-generation cephalosporin), cefuroxime, cefamandole and cefoxitin (2nd generation cephalosporins) have been widely recommended with success. Third generation cephalosporins, such as cefotaxime, cefoperazone, ceftriaxone, ceftazidime or ceftizoxime are generally not recommended for surgical prophylaxis.[27] Despite these recommendations, the results of our survey showed that ceftriaxone and cefuroxime were commonly preferred for surgical prophylaxis. Our survey thus clearly reveals that antimicrobials are being over prescribed in number as well as days of usage, especially for surgical prophylaxis. Many hospitals have attempted to address these issues by establishing Hospital Infection Control Committees (HICC), to lay down guidelines and streamline antimicrobial usage. Our survey results showed that less than half the respondents' Institutions had an HICC. However, only 8.5% surgeons in case of clean surgeries, 4% in case of clean contaminated surgeries and none of the surgeons in case of dirty surgeries were prescribing as per the guidelines. Thus, presence of an HICC did not seem to impact prescribing trends. The present survey does have its limitations in the point that the day to day prescribing habits of the surgeons may be different from that put down on paper for the survey and rationality of the prescription cannot be assessed without patient details. CONCLUSIONS The high use of antimicrobials especially for a prolonged duration is a matter of concern. There is an urgent need to promote rational antimicrobial prescribing among surgeons. The need of the hour is developing and implementing consensus-based national guidelines for treatment of surgical infections and prophylaxis by a multidisciplinary group of experts.References
Copyright 2005 - Indian Journal of Surgery The following images related to this document are available:Photo images[is05093t2.jpg] [is05093t4.jpg] [is05093t1.jpg] [is05093t9.jpg] [is05093t3.jpg] [is05093t8.jpg] [is05093t5.jpg] [is05093t6.jpg] [is05093t7.jpg] [is05093f1.jpg] |
| |||||||||

{kind=link}