 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 68, No. 1, January-February, 2006, pp. 17-22 Original Article Colour flow doppler: An emerging alternative to conventional arteriography for arterial mapping in peripheral arterial occlusive disease Thakur RajeshwarSingh, Minhas SS, Dhiman DS*, Abbey RK Department of General Surgery, IGMC Shimla, HP, *Department of Radiology, RPGMC Tanda, HP, India Code Number: is06003 Abstract Background: Arteriography has been considered the "Gold Standard" for the investigation of Peripheral arterial occlusive disease (PAOD). The development of Colour flow Doppler (CFD) has extended the scope of non-invasive assessment of chronic lower limb arterial disease.Aims: To evaluate and correlate the findings of CFD with arteriography as the gold standard, in PAOD of the lower extremities. Settings and Design: This prospective study was designed in the department of general surgery IGMC, HP. Patients were subjected to CFD scan followed by arteriography, to evaluate the aorto-iliac and femoro-popliteal vessels. Materials and Methods: Thirty patients of PAOD formed the subjects and their affected lower limbs evaluated by CFD and arteriography, for localization and grading of lesion in the arteries, into normal/insignificant stenosis, significant stenosis and occlusion. The results were analyzed in a blind fashion in a total of 45 limbs comprising of 300 vascular segments. Statistical Analysis: Results were analyzed by two way contingency tables and kappa statistics. Results: CFD was able to identify 50 of the 59 (85%) lesions identified on arteriography. There was good statistical agreement and sensitivity of CFD ranged from, 80% to 100% and specificity from 93.9% to 100% in different arterial segments. Conclusions: CFD has grown from an ancillary diagnostic aid, to a critical component in the non-invasive diagnostic workup for patients with PAOD of the lower extremity, with the potential of displacing arteriography as the primary diagnostic imaging modality. Keywords: Peripheral arterial occlusive disease, colour flow doppler, arteriography The diagnosis and management of peripheral arterial occlusive disease (PAOD) is based on careful history, physical examination and a variety of diagnostic tools. Arteriography has been considered the "Gold Standard" for the investigation of PAOD, as it provides anatomical details not obtained from other imaging techniques.[1],[2] Arteriography is however vulnerable as a gold standard, as it is invasive, costly and associated with small but significant morbidity, which limits its utility, particularly as a screening modality.[3],[4] Furthermore it is subject to interpretational variability.[5],[6] Moreover the eccentric nature of many lesions may result in arteriography underestimating the extent of disease.[7],[8] Colour Flow Doppler (CFD) provides high-resolution, precise anatomical & physiological information of the peripheral arteries and so the movement of blood flow can be accurately detected by this technique.[9],[10] It consists of three components; B-mode ultrasound for road mapping , pulse Doppler ultrasound for spectral wave-form analysis and velocity estimation and colour Doppler for rapid assessment of vessel patency, abnormal and normal flow, which in turn guides the placement of pulsed Doppler. CFD is a safe, fast, inexpensive, accurate and repeatable non-invasive procedure and is being used more frequently as the first line of investigation for patients presenting with symptoms of chronic arterial occlusive diseases of lower limb.[10] In view of the limitations of arteriography and the present trend of opting for noninvasive diagnostic modalities, this study was undertaken so that this technique can be used beyond its present role as an ancillary diagnostic aid. Materials and Methods The present prospective study was undertaken in the department of surgery, Indira Gandhi Medical College, Shimla Himachal Pradesh. Thirty patients of peripheral arterial occlusive disease of the lower extremity, admitted in the surgical wards during the period from March 03 to June 04 formed the subjects and their affected limbs subjected to evaluation. The diagnosis was based on comprehensive history, suggestive of peripheral arterial occlusive disease and signs of chronic lower limb ischemia on physical examination. The following patients were excluded from the study:
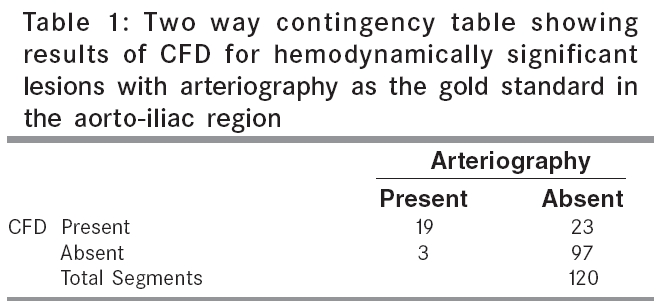
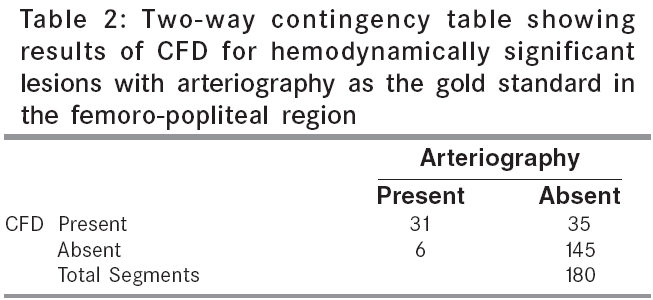
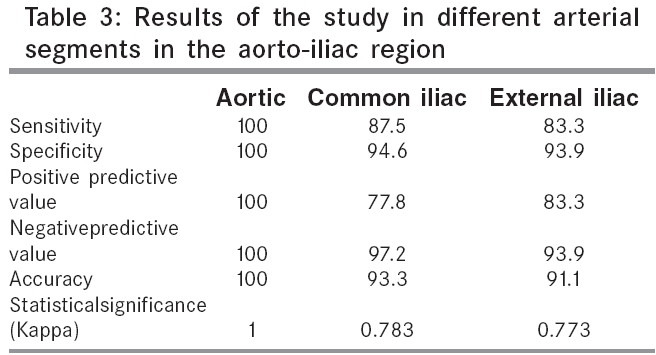
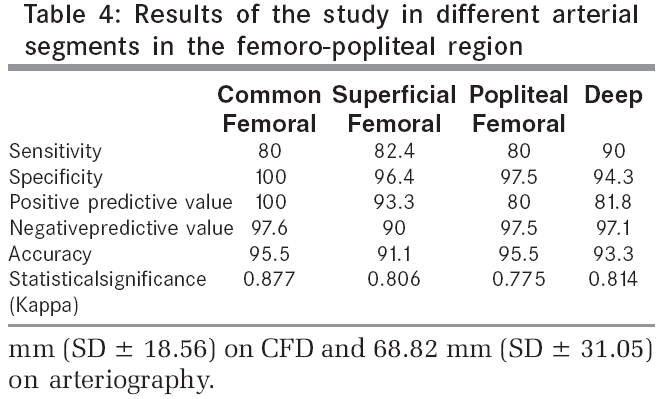
Written consent of each patient was recorded on the prescribed proforma. The patients were subjected to colour flow Doppler scan of symptomatic limbs, followed by arteriography for localization and classification/grading of lesion in the arteries into normal/insignificant stenosis (0-49%), significant stenosis (50-99%) and occlusion (100%), length of lesion and distal run-off. CFD scan of symptomatic limbs was performed by a radiologist on a Toshiba core vision scanner, having band width frequency transducer with a range of 6-12 MHz (selective frequency 6, 8 and 10) and 2-6 MHz (selective frequency 3.75), respectively. Patients were kept fasting for at least 6 hours, to improve visualization of the aorto-iliac region, the access to which is hindered by the overlying bowel gases. Angle of isonation was kept close to 60 degree to the vessel axis. Colour flow assisted B-mode was used to rapidly map the vessel of interest and locate lesions, followed by use of gray scale sonography to identify morphological features. Pulse Doppler was then used to analyze spectral waveform and to measure peak systolic velocity. Arterial lesions were located by change in colour flow pattern, change in vessel diameter and broadening of Doppler spectrum, whereas stenosis was quantified by increase in peak systolic velocity (PSV). Patency of vessel was determined by normal triphasic waveform pattern and colour saturation, demonstrated throughout the lumen of the artery. Occlusion was diagnosed, when no colour saturation and no Doppler waveform was seen in the artery. A hemodynamically significant stenosis was inferred when the waveform changed from triphasic to monophasic, with appearance of spectral broadening and increase in peak systolic velocity. Doubling of peak systolic velocity with respect to a point with normal flow pattern in the lumen at least 4 cm proximally expressed, as peak systolic velocity ratio. Peak systolic velocity ratio of ≥ 2 was used as a criteria for significant stenosis.[2],[11],[12],[13] Length of the lesion was recorded in millimeters and duration of evaluation recorded in minutes. Cine arteriography was performed under fluoroscopic guidance, using percutaneous Seldingers technique.[14] Sixty to eighty ml of non ionic contrast agent, Ioxehol (Omnipaque) was injected through the pigtail catheter, by pressure injector at the aortic bifurcation. In some cases selective hand injections were given through 6 French right coronary catheters into the right and left common iliac and was then followed into the distal vessels, to know the presence of the lesion and its anatomical distribution. To avoid bias, Colour flow doppler was done by a radiologist before arteriography. Arteriography was in turn done by a cardiologist, who was unaware of the findings of CFD and the findings recorded in a prescribed proforma. The results of CFD scan and arteriography were analyzed independently by the third observer, in a blinded fashion in the following vascular segments; Infra-renal aorta, common iliac and external iliac artery in the aorto-iliac region and common femoral, superficial femoral, origin of deep femoral artery and popliteal artery in the femoro-popliteal region. Thus, for a patient with unilateral limb involvement, seven segments were examined and in case of bilateral limb disease, thirteen segments were examined. In all 45 limbs, a total of 300 vascular segments were studied. Statistical analysis Results Colour flow doppler revealed 58 diseased segments out of which 6 were stenotic and 52 occlusions. Arteriography revealed a total of 59 diseased segments,out of which 4 were stenotic and 55 were occluded. In all, CFD was able to identify 50 of the 59 (85%) hemodynamically significant lesions identified on arteriography. Aorto-iliac region: Aorto-iliac region was the most difficult region to access, as the overlying gases in the gut and excessive abdominal movement made the process of identifying and analyzing the vessels difficult, as reported earlier.[12] Colour flow Doppler was able to correctly pick up 16 of the 19 occlusions and all the 3 stenosis identified on arteriography. There were 2 false positive occlusions, (one each in the common iliac and the external iliac segments,) and 2 false positive stenosis, (one each in the common iliac and the external iliac segments). There were 3 false negative occlusions,(one in the common iliac & two in the external iliac segments) and no false negative stenosis. On analysis with arteriography as the gold standard, sensitivity ranged from 83.3% to 100% and specificity from 93.9% to 100%, in different arterial segments. The results of sensitivity, specificity, PPV (ranged from 77.8% to 100%), NPV (ranged from 93.9% to 100%) accuracy (ranged from 91.1% to 100%) and statistical significance for hemodynamically significant lesions versus patent segments for each segment are tabulated in [Table - 3]. On statistical analysis, results showed perfect agreement in the aortic segment (Kappa:1) and excellent agreement in the other two segments (Kappa:≥ 0.75).[15] P value was < 0.001 which is highly significant. Femoro-Popliteal region: This region, being superficial, was easier to scan, except for the deep femoral artery beyond its origin, where it becomes deep. Distal third of the superficial femoral artery, which lies deep in the hunter canal, was the most difficult to visualize, due to its deep course, which causes decreased penetration of the ultrasound beam, as has also been reported in literature.[12] Popliteal artery needs to be properly assessed, to verify that no significant lesion exists proximally in the adductor canal, if the entire course of the adductor canal cannot be visualized.[10] CFD correctly identified 30 of the 36 occluded segments and a single stenotic segment identified on arteriography. There were 4 false positive occlusions (one in superficial femoral, one in the deep femoral and two in the popliteal) and 6 false negative occlusions (one each in the common femoral, deep femoral, popliteal and three in the superficial femoral segments). There were no false positive or false negative stenoses. Sensitivity ranged from 80% to 90%, specificity from 94.3% to 100%, PPV ranged from 80% to 100%, NPV ranged from 90% to 97.6% and accuracy from 91.1% to 95.5%, in different arterial segments. The results are tabulated segment wise in [Table - 4]. On statistical analysis, results when analyzed, showed that with P value of < 0.001. Kappa was ≥ 0.75 in all the vascular segments which represented excellent agreement.[15] CFD underestimated the overall length of the occlusive lesion, compared to arteriography in most of the patients, with mean length of occlusion being 50.88 mm (SD ± 18.56) on CFD and 68.82 mm (SD ± 31.05) on arteriography. Arteriography revealed distal runoff for bypass grafting in 21 limbs, whereas triplex scan was able to pick runoff in 23 limbs, inclusive of the limbs picked up on arteriography i.e. there were two false positive results. The sensitivity and specificity to identify runoff was 100% and 91.6%, respectively and with two false positive results, the overall accuracy was 95.5% Moreover, CFD scan was able to identify additional morphological features, such as presence or absence of plaques and whether these were soft, mildly calcified or heavily calcified. In this study, time taken was more for the initial scans done, when the study was started and gradually decreased, as more experience was gained over the period. Mean time for single limb scan was 36.8 minutes (S.D.± 8.81) and for both limb scan was 58 minutes (S.D.±12.46), which is more than reported in literature.[10],[11] This was because of the initial learning curve of our sonologists. However, time taken, approached the comparable value towards the end of the study, as experience was gained. Discussion The status of arteriography as the ′gold standard′, is derived from its long established, tried and tested place in clinical practice, rather than its inherent merits. Comparative studies with other diagnostic modalities have been based on this assumption, which is unfortunate, because it means that Doppler ultrasound can be only the second best. Our results show good statistical agreement between the findings of CFD and arteriography in both the aorto-iliac as well as femoro-popliteal region, for identifying hemodynamically significant lesions, with the kappa ranging from. 773 to 1, which represents excellent to perfect agreement.[15] Sensitivity ranged form 80% to 100%, specificity 93% to 100%, PPV from 77% to 100%, NPV from 90% to 100% and accuracy from 91% to 100%, in different vascular segments. CFD is able to identify distal runoff well and can also comment upon the morphological features of vessel wall. False positive occlusions: These are reported to occur due to sluggish low velocity flow, with most of the blood being diverted away from the main vessel by the collaterals, decreasing the amount of blood carried by it, which is not picked up by doppler with the overlying gases in the bowel, movement of abdominal wall due to respiration and heavily calcified vessel wall, leading to beam attenuation, further compounding the problem.[12] It is also reported to be due to diffuse insignificant proximal disease.[10] Moreover, distal third of the superficial femoral artery has been called a blind spot for sonographers. False negative occlusions: This phenomenon of non visualization of patent segments on Doppler, is known and reported in literature and has been demonstrated in other studies.[2],[16] This non- opacification of normal segment distal to occlusion, is said to be due to its filling with non opacified blood from the collaterals, not carrying the contrast due to timing, or flow or pressure variables. The results are misleading, leading to overestimation of occlusion lengths and at times, revealing no runoff on arteriography and subsequent selective arteriography, or observations at surgery tend to substantiate the findings of the CFD.[2] Vascular surgeons have known this for a long time and will explore non-visualized distal vessels for distal bypass grafting, if Doppler is detectable. This shows that our observed sensitivity can be deceptively lower. Moreover arterial collateral branch can also be inardventely sampled as the patent main arterial segment,as reported literature.[10],[12],[17] False positive stenosis: This possibly occurred due to sampling error, as narrowing was not appreciated on the colour scan and spectral waveform in the distal vasculature was tri-phasic, whereas abnormal spectral waveform should continue in the distal vessels.[13] More experience in the future will avoid such errors. The present study however has its limitations, in that the infra-popliteal region was not included in the study. The study could have been further strengthened, if the findings could have been compared with the operative findings in cases requiring bypass grafting. Moreover, there were only 5 stenotic lesions and a larger sample could have given better outcome and stenotic and occlusions could have been studied separately. Thus, CFD can facilitate the pre-angiographic determination of the nature and extent of arterial disease in the lower limbs. Normal CFD virtually excludes significant lesion, which in turn helps reducing the number of unnecessary diagnostic arteriography in patients with symptoms not justifying the surgical or endovascular procedure. The decision of whether or not to proceed for angiography, can be taken on the basis of results of CFD and treatment plans can be formulated prior to arteriography, as CFD provides sufficient information as whether to proceed to endovascular intervention or surgery. The road map of the arterial tree inferred from pre- angiographic CFD can be helpful to the angiographer to tailor the angiographic technique for the patient. Moreove, the angiographic approach can be determined beforehand, as the road map of the arterial tree inferred from the pre- angiographic CFD is already at hand. The accuracy and time spent obtaining the arteriograms are also improved, by obviating the need to look for lesions where they do not exist. In addition, examination time is decreased and contrast load diminished if portions of the arterial system can be shown normal on CFD. CFD is also a more accurate way to access the exact length of an occlusion than arteriography, the latter tending to overestimate the length of the lesion. Cautious approach is required in undertaking operative or catheter based procedures in the treatment of PAOD, on the basis of triplex scan results alone, till more experience is gained. However, in the event of triplex scan revealing stenotic lesion, angioplasty can be planned at the time of routine arteriography, combining diagnostic and therapeutic intervention in the same sitting. In patients needing femoro-distal reconstruction, diagnostic arteriography is still recommended in planning operative treatment. Our results are in good agreement with the earlier studies.[11],[12] Koelemay et al,[18] in their review article, concluded that CFD is an excellent tool in the noninvasive work up of patients with PAOD, in aortoiliac and femoropopliteal segment. Because of its high diagnostic accuracy, it can replace routine diagnostic arteriography for planning surgical intervention or PTA in a substantial number of patients. For assessment of infra-crural arteries, angiography remains a pre-requisite and our results seem to substantiate this. However, more experience is required before we venture on therapeutic decisions on the basis of this emerging new tool of non invasive mapping of the peripheral vasculature, though there is evidence in literature to favour the contrary.[19],[20]A study has concluded, that CFD can replace diagnostic arteriography in up to 97% of lower limb disease.[20] However, in future, more studies need to be undertaken to firmly establish the role of CFD as a primary diagnostic modality. Conclusion Colour Flow Doppler has reached the diagnostic standard of arteriography and provides high-resolution, precise anatomical and physiological information of the peripheral arteries. It is a safe, fast, inexpensive and repeatable non-invasive procedure for investigating PAOD, which can be performed on outdoor basis without hospital admission. With arteriography as the ′gold standard′, deceptively poor results can be produced, due to non-visualization of segments patent on CFD. A high NPV shows that significant lesions in the vascular tracts can be reliably excluded, which can help reduce the number of diagnostic angiographies, in patients with symptoms not justifying a surgical or endovascular procedure. The study found that, when scan demonstrates normal artery, the angiogram also shows normal segment. Thus, CFD has grown from an ancillary diagnostic aid, to a critical component in the diagnostic workup, raising the possibility of displacing arteriography as the primary diagnostic imaging modality, for patients with chronic arterial occlusive disease of the lower extremity.References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06003t1.jpg] [is06003t4.jpg] [is06003t3.jpg] [is06003t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}