 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 68, No. 1, January-February, 2006, pp. 23-26 Original Article Missed malignancies at laparoscopic cholecystecomy: A new emerging problem Jain N, Tewari M, Shukla HariS Department of Surgical Oncology, Institute of Medical
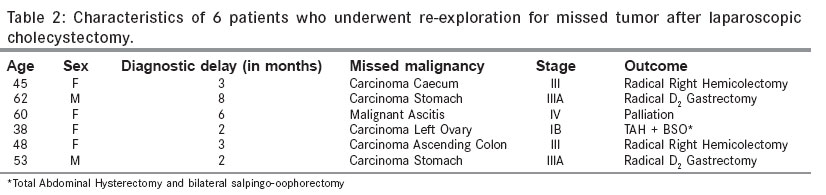
Sciences, Banaras Hindu University, Varanasi Code Number: is06004 Abstract Objective: With increase in laparoscopic cholecystectomy (LC) rates the chances of missing a concomitant cancer is high, if the laparoscopic surgeon is focused on gall bladder and does not look around. The aim of the present article therefore is to analyze the unsuspected concomitant cancer, for patients with atypical upper abdominal symptoms and diagnostic delay due to LC.Materials and Methods: This retrospective study evaluates the clinico- pathological data, diagnostic delay and outcome of patients who presented with intra-abdominal malignancy to our unit within 2-8 months of LC for gallstone disease elsewhere, between June 2003 and June 2005. Results: Six such patients were identified (age range 38-62 years). Two patients had carcinoma of the stomach, one each had carcinoma of the caecum, ascending colon and left ovary respectively, while one patient presented with malignant ascitis of unknown origin. Five of these 6 patients underwent a subsequent radical oncological procedure at our unit. Mean diagnostic delay was 4 months. The cTNM of tumor at diagnosis was Stage III/ IV in 5 of these 6 patients. Conclusion: The importance of a good clinical work-up, diagnostic imaging studies and exploration at the time of surgery is re-emphasized. Missing a concomitant lesion is high, if the surgeon focuses only on one organ during an LC. Keywords: Missed malignacies, laparoscopic cholecystectomy, emerging problem The safety and efficacy of laparoscopic cholecystectomy (LC) is now widely accepted for benign gall bladder diseases and has resulted in increasing number of cholecystectomies being performed. [1],[2],[3],[4] The benefits of LC are obvious in relation to reduced post operative pain, more rapid convalescence and better cosmetic results.[5],[6] A serious, albeit less frequently reported hazard of LC is a missed underlying pathology [Table - 1]. [6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23],[24] This article reports the case histories, diagnostic delay and the resultant impact on the patient′s prognosis due to an intra-abdominal malignancy missed in 6 such patients during LC outside our unit. The available reports on missed diagnosis after LC from indexed medical literature are also reviewed and discussed. Materials and Methods The data of all patients who had undergone LC elsewhere for suspected gall stone disease and then were either referred or presented themselves for various reasons to the Department of Surgical Oncology between June 2003 and June 2005, were reviewed from our own department′s patient′s follow up record books. Of these, patients diagnosed as having an intrabdominal malignancy within 2-8 months of LC were sorted out. The age, sex and clinical symptoms at presentation to our unit, that prior to LC and the delay in diagnosis of a malignancy missed at LC elsewhere, were recorded as mentioned in the records. A thorough staging evaluation of each of these patients was carried out followed by a standard oncological procedure and adjuvant/ palliative therapy at our unit. The outcome of the patients was also retrospectively analyzed. Results In all, six patients with an intra-abdominal malignancy within 2-8 months of LC elsewhere, were identified from 46 patients who were admitted for various reasons following LC outside our unit, between June 2003 and June 2005. The age of the 6 patients selected, ranged from 38 to 62 years, with mean age of 51± 9.16 years. Among the 6 patients, 4 were female and 2 male. Five of these 6 patients required re-exploration for malignant tumor missed at LC, while one was managed non-surgically. All six patients had complained of atypical upper abdominal pain before LC elsewhere. An abdominal ultrasonography and histology (done outside our unit), had revealed chronic cholecystitis in all these 6 patients. The diagnostic delay ranged from 2-8 months (mean 4 months). The site of the malignant tumor, diagnostic delay and outcome is summarized in [Table - 2 ]. Five patients underwent curative resection, while one patient was diagnosed to have advanced cancer and was managed with palliative chemotherapy and supportive care. Case 1 The patient was referred to Department of Surgical Oncology, 3 months following LC, with complaints of weight loss and blood mixed stools. Abdominal computed tomography and colonoscopy at our department showed a circumferential tumor in caecum. The Carcinoembryonic Antigen (CEA) level was within the normal range. After the colonoscopic biopsy confirming an adenocarcinoma, a radical right hemicolectomy was performed. The histology revealed it to be a well differentiated adenocarcinoma of the caecum with metastasis to 4 of 12 regional lymph nodes (Dukes C). She also received standard 6 courses of adjuvant chemotherapy (5-Fluorouracil 425 mg/m2 D1-5, given after Folinic acid 20 mg/m2 D1-5 x q 4 weeks). Case 2 Case 3 Case 4 Case 5 Case 6 Discussion Since its first description in 1985, the technique of LC has undergone great technical refinements, as well as general acceptance for uncomplicated and complicated cholelithiasis. A potential disadvantage of LC is its lost ability to palpate abdominal organs, which the formal laparotomy of open cholecystectomy previously allowed. It appears that the enthusiasm with which LC is now performed, has led to labelling of anyone who presents with right upper abdominal pain and a positive ultrasound, as having symptomatic cholelithiasis. Asymptomatic gallstone or those discovered incidentally, generally require no further treatment, but with the advent of LC, its application has increased inadvertently. The six patients that we are reporting, highlight the emerging problem of missed malignancies during LC. In our study, the delay in diagnosing malignancy was between two to eight months, post LC. Fortunately, a curative radical resection was still possible in 5 patients. The stage at presentation was advanced in the majority, with a relatively short delay in diagnosis. It can be emphasized further, that as a cancer grows rapidly, even a small delay can be detrimental. There have been reports of missed malignancies at the time of LC, in the world literature but the incidence has infrequently been quantified. According to related articles describing cancer missed during LC [Table - 1], the delay in diagnosis ranged from 2 weeks to 24 months and majority of tumors were advanced at presentation and the mean incidence of missed intra abdominal pathologies is 0.65%. Patients with atypical symptoms or unusual findings warrant a more detailed preoperative assessment of alternative etiologies, as the resultant delay in the diagnosis of cancer obviously upstage the tumor at the time of presentation and decrease its potential curability, hence overall survival benefit. Should patients under going LC be investigated more thoroughly preoperatively, more intense investigation would probably be of benefit in a small number of patients and thus would not be cost effective. Rickman concluded that the risk is small and that abdominal exploration at the time of treatment of cholelithiasis is unnecessary.[26] The National Institute of Health Consensus Conference on Gall-stone, emphasized that patient of cholelithiasis with atypical pain or dyspepsia needs further investigation to determine the cause of their symptoms.[27] Open mini-cholecystectomy allows minimal access to other organs and perhaps offers a greater disadvantage than a formal Kocher′s incision, or even a LC. Its use may not be advisable in all patients, especially when diagnosis is doubtful. Conclusion This study emphasizes that the success of a treatment should not be compromised to merely utilize the minimally invasive approach. A careful evaluation of each patient, especially the elderly and those with atypical symptoms, along with good visualization of the neighboring organs may aid in preventing such iatrogenic complications in future. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06004t1.jpg] [is06004t2.jpg] |
| |||||||||

{kind=link}
{kind=link}