 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
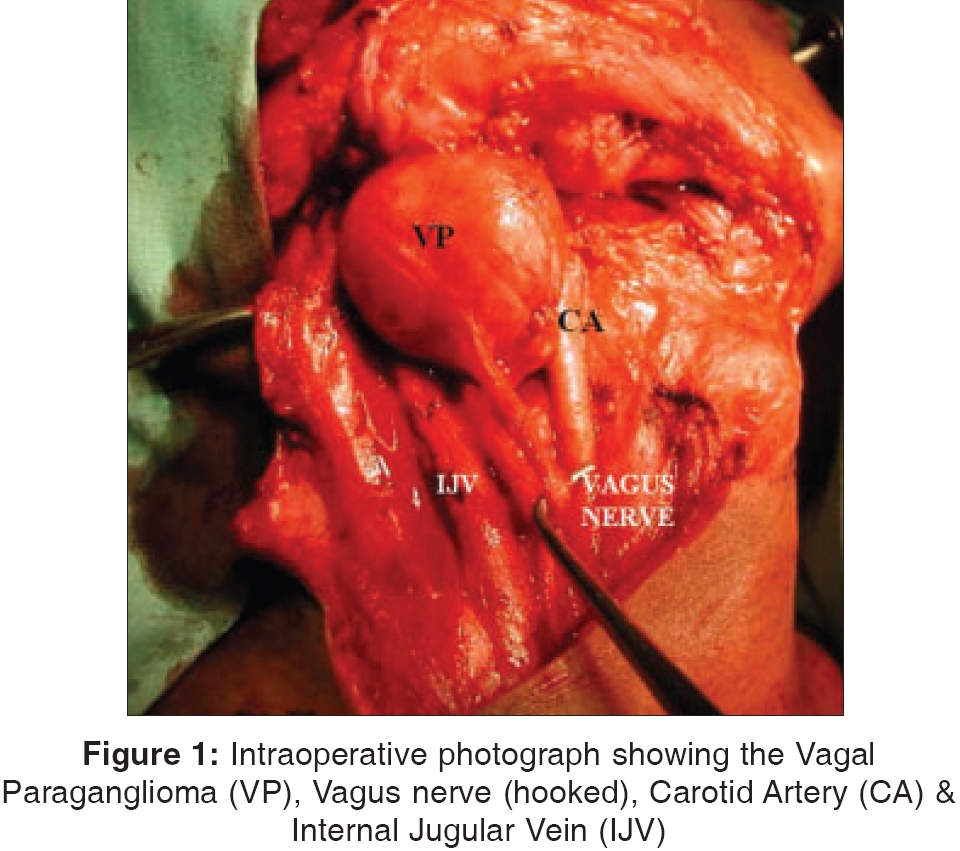
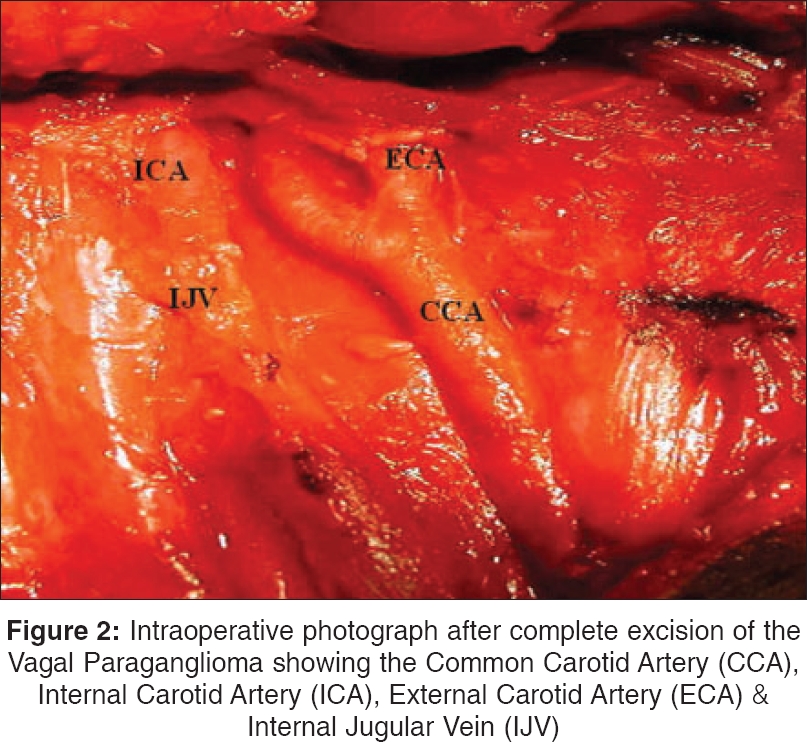
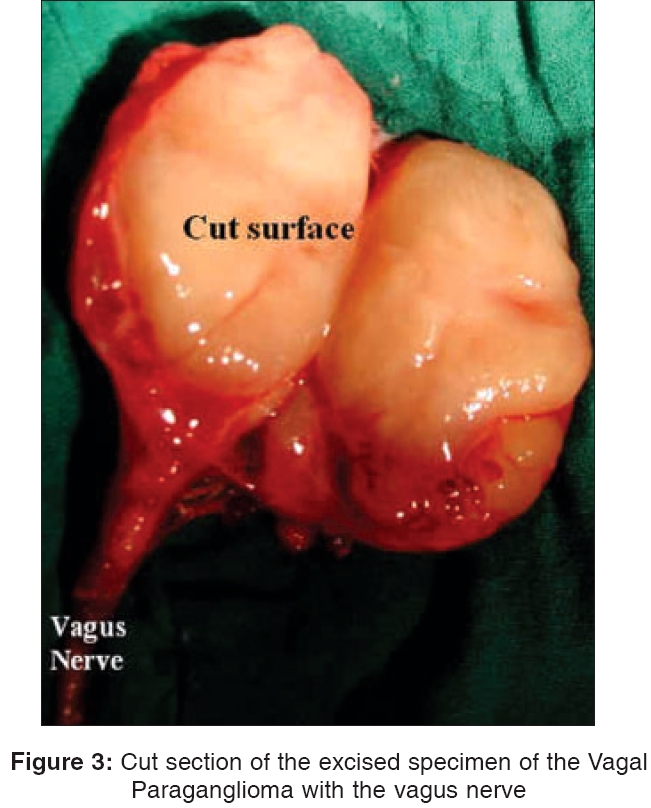
Indian Journal of Surgery, Vol. 68, No. 1, January-February, 2006, pp. 30-32 Case Report Vagal paraganglioma M. Tewari*, V. Srivastava, H. S. Shukla* *Department of Surgical Oncology Institute of Medical Sciences, Banaras Hindu University, Varanasi and RRC* Varanasi, India Code Number: is06006 Abstract Vagal paragangliomas (VP) arise from paraganglia associated with the vagus nerve. Approximately 200 cases have been reported in the medical literature. The management of VP is associated with partial or total loss of vagal function. We report a case of VP in a young boy who presented with neck mass associated with recurrent laryngeal nerve paralysis. Evaluation of the patient was done by laryngoscope and ultrasound examination of the neck. The paraganglioma was excised along with the vagus nerve with ipsilateral loss of vagal function.Keywords: Paraganglioma, vagus, neck Introduction Vagal paragangliomas is a rare tumor of neural crest origin. In 1935, Stout identified the first paraganglioma of the vagus nerve and Birrell proposed the term vagal body tumor in 1953. VP most commonly arises from glomus tissue rests within the inferior (nodose) ganglion. Other locations include the superior ganglion or elsewhere along the course of the vagus nerve.[1] Although the literature is in agreement with regard to epidemiology, diagnosis, tumor biology, there is some controversy over treatment modalities for these patients. We report the observation of one case of VP in a young boy that was surgically treated. Case Report A 17-year boy presented to us with 8 months history of a painless neck swelling just below his right jaw. He had developed hoarseness of voice for 3 months. Examination revealed an 8 cm x 6 cm oblong, non-tender, non-pulsatile, firm mass in the upper part of the carotid triangle. It was mobile in the horizontal axis. The carotid was displaced anteromedially. No lymph nodes were palpable. B-mode ultrasonography of the neck revealed a hypoechoic solid mass localised in the carotid triangle. Colour Duplex ultrasonography (CDS) showed the lesion to be hypovascular with the carotid artery displaced anteromedially and internal jugular vein (IJV) posterolaterally. The diagnosis of VP was made. Laryngoscopy revealed paralysis of right cord. A longitudinal incision was made along the anterior border of sternomastoid muscle. Careful dissection revealed 6cm smooth rounded tumor arising from the vagus nerve [Figure - 1]. It was excised [Figure - 2]. The cut surface was fleshy solid and smooth [Figure - 3]. Histology showed it to be VP. Postoperatively the patient developed nasal regurgitation of food for 4 weeks. Follow-up 18 months after surgery showed no recurrence. There was no disability other than persistence of hoarseness of voice. Discussion The paragangliomas make up a family of neoplasms that develop from paraganglia tissues (chemoreceptor organs) distributed throughout the body. The most common location in head and neck is the carotid body, followed by the jugular bulb and vagus nerve.[2] VP (5% of paragangliomas) is a distant third in terms of prevalence.[1] These are slow growing and often present as asymptomatic cervical masses.[3] Vagal nerve deficits are seen late in the clinical course of these lesions, as the fibers of the vagus nerve are usually splayed over the surface of the tumor. Other lower cranial nerve palsies from hypoglossal, accessory or glossopharyngeal involvement commonly occur as late manifestations, typically 2 years after initial presentation (20-50%).[1] Homer syndrome with infiltration into the cervical sympathetic chain occurs in 25% of patients. Rare manifestations include isolated hoarseness or vocal cord paralysis, as was in our patient. Approximately 10% are bilateral.[4] About 7- 15% are malignant[5] and may metastasise to regional lymph nodes or distant sites, commonly lungs and bones. Diagnostic work up includes CT/MRI and lately CDS and in selected situations, angiography. MRI is superior to CT in assessing intracranial extension, as well as the relation of tumor to bone. The VP displaces both the External carotid artery (ECA) and Internal carotid artery (ICA) anteromedially, separating these vessels from the IJV. On arteriography tumors located high on the nerve, tend to displace ICA anteriorly. Carotid body tumors, on the other hand cause splaying of ICA and ECA. It can now be seen via non-invasive CDS,[6] as in our patient. Treatment includes surgical resection, radiation therapy and in selected cases observation only. Traditionally the mainstay of treatment has been surgical removal. In general, young patients with small tumors are treated surgically. Patients with unresectable tumors, residual tumor following surgery, tumor that occludes the ICA, who refuse surgery or those who are unsuitable surgical candidates, radiation therapy may serve as an excellent palliative modality.[7] Complications associated with surgical extirpation of VP include cranial nerve paralysis (67% of cases), especially involving the vagus nerve.[1] The tumor in our patient was successfully completely excised surgically. Malignant paragangliomas are managed most effectively with either surgery or radiotherapy or a combination of both. Chemotherapy has no defined role for treatment at any stage.[8] Conclusion The management of VP is a difficult clinical problem as the diagnosis is at times difficult and its treatment is associated with cranial nerve paralysis. Rehabilitation for hoarseness of voice and nasal regurgitation is required for mid-cervical VP.References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06006f3.jpg] [is06006f2.jpg] [is06006f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}