 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
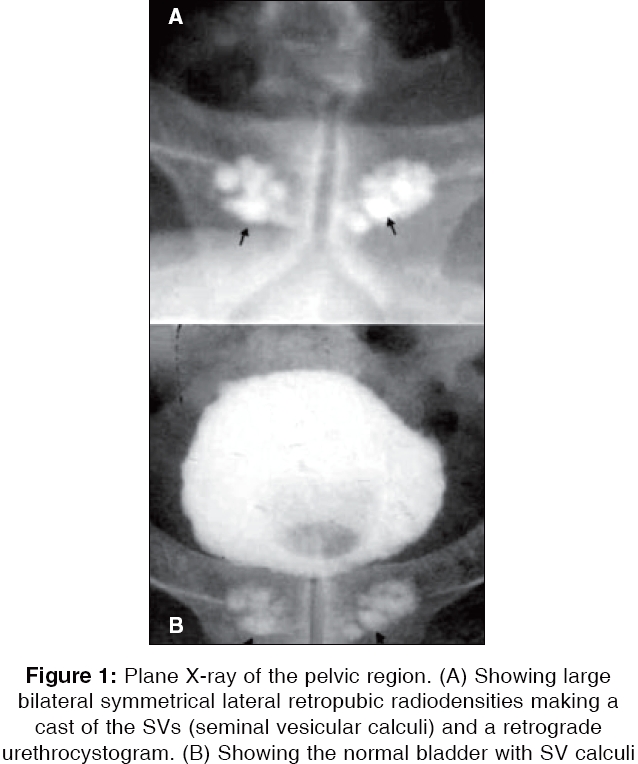
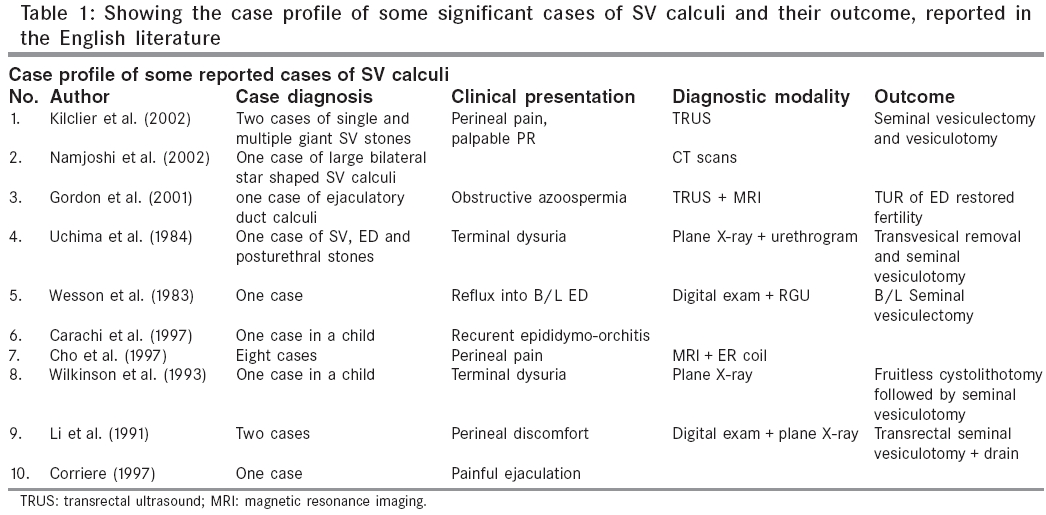
Indian Journal of Surgery, Vol. 68, No. 1, January-February, 2006, pp. 38-40 Case Report Idiopathic bilateral giant seminal vesicle calculi and calcification of the male ejaculatory system: Current review of diagnosis and management Singh Iqbal, Ansari MS* Department of Surgery, University College of Medical Sciences and G.T.B. Hospital, and *Department of Urology, AIIMS, New Delhi, India Code Number: is06009 Abstract Seminal vesicular lithiasis or seminal vesicular and ejaculatory duct calculi or calcification are rarely encountered with very few cases reported in the literature. We aim to present and review the literature of one such case. A search of the published English literature revealed only 20 published case reports of seminal vesicle calculi, with only three attributed to large bilateral seminal vesicle calculi, making the present case to be the fourth such case. A young man with loin pain and dysuria was investigated and found to have idiopathic giant bilateral seminal vesicular calculi. Stones of the seminal vesicle and ejaculatory duct apparatus are rare and difficult to diagnose. Their presentation may be diverse ranging from a spectrum of loin pain to infertility, hemospermia, painful ejaculation to epididymo-orchitis and urinary tract infection. Transrectal ultrasound and or magnetic resonance imaging should be performed whenever a high index of clinical suspicion persists, in order to arrive at a definite diagnosis. Symptomatic younger patients respond to seminal vesiculectomy whilst in the elderly seminal vesiculotomy may suffice.Keywords: Ejaculatory duct calculi, seminal vesicle calcification, seminal vesicular calculi, urinary tract stones; urolithiasis A 35-year-old fertile man presented with complaints of increased frequency of micturition, dysuria, and lower abdominal pain for the past several months. There was no history of hematuria, hemospermia, urinary tract infection, pyuria, and graveluria. The digital rectal examination was unremarkable. The urine and semen routine analysis/culture/acid-fast bacilli, blood sugar, renal function tests, and serum PSA were within normal limits. There was no evidence of hypercalcemia or any other related metabolic abnormality. The uroflowmetry did not reveal any evidence of outflow obstruction. X-ray KUB revealed bilateral large bean-shaped lateral pelvic retropubic radiodensities suggested of vesical and or seminal vesicle (SV) calculi measuring approximately 4 x 3 cm 2. The calculi were multiple located in the intra SV lacunae almost making a cast of the SV. A transrectal ultrasound and a contrast-computed tomography scan of the SV, ejaculatory ducts and prostate confirmed retrovesical location of the SV stones (mean core radio density being over 1000 hounsfield units) thereby eliminating any possibility of SV calcification. A voiding cystourethrogram [Figure - 1 ] confirmed seminal vesical calculi and ruled out any evidence of neurogenic bladder, vesicoureteral reflux, or reflux into the ejaculatory ducts. The patient declined a seminal vesiculectomy. Discussion Seminal vesicular and or ejaculatory duct calculi or calcification are extremely rare with very few cases reported in the literature.[1],[2],[3],[4],[5],[6],[7],[8],[9] Common symptoms range from asymptomatic to perineal[1] or testicular[5] pain, hemospermia,[2] painful ejaculation[8] and low volume ejaculates.[1],[2],[3],[4],[5],[6],[7],[8],[9] Rarely reflux into the ejaculatory ducts[5] and epididymo-orchitis[6] has also been described, which may be the cause of severe testicular and or perineal pain. Seminal vesiculitis due to stasis and diabetes has been the most important known etiological factor in a majority. Certain other serious underlying conditions that may be associated with SV calcification/calculi includes SV cysts/hypoplasia, obstructive azoospermia/infertility/hemospermia, chronic prostatitis, genitourinary tuberculosis, SV and prostatic schistosomiasis, cancer prostate/SVs and metatstatic calcification of diverse etiology. These should be looked for and treated since these may not form a part of the early presentation.[9] Analysis of the SV stones by infrared spectroscopy has revealed magnesium-ammonium-phosphate thereby corroborating their infectious etiology; however, in the present case no definite cause could be ascertained. In the present case, there was no evidence of obstructive uropathy, urosepsis, urinary tract infection, neurogenic bladder, diabetes, tuberculosis, or reflux into the SV/ejaculatory ducts. Nevertheless, one must diligently search for and rule out the known conditions associated with SV calcification/calculi. [Table - 1 ] shows the diverse profile of some significant cases reported in the English literature. The diagnosis of SV calculi is generally suspected on a combination of a triad of clinical symptoms, digital examination, and a plane X-ray.[4],[7] A retrograde urethrogram/voiding cystourethrogram may be needed at times especially in the children to distinguish them from vesical and or posterior urethral calculi. Confirmation of SV calculi is currently made on the basis of transrectal ultrasound (TRUS) and magnetic resonance imaging (MRI) with an endo-rectal surface coil. The TRUS has an established role in the detection, differential diagnosis and confirmation of genitourinary pathologies (cysts and tumors) of the prostate, SVs, and ejaculatory duct. The TRUS should be freely considered for the evaluation of significant genitourinary symptoms that may previously have been ascribed to prostatodynia, chronic nonbacterial prostatitis or have been considered to be idiopathic. In case of symptomatic cystic lesions of the SV, TRUS serves the dual benefit of guided aspiration/sclerotherapy that may be curative. In cases where TRUS fails or is unsatisfactory, MRI remains a highly effective noninvasive modality to evaluate the seminal tract of patients with bothersome genitourinary symptomatology. In the present case, although the patient declined any surgical extirpation, the recommended therapy includes laparoscopic/open seminal vesiculectomy in the young, and seminal vesiculotomy in the elderly.[3] For SV stones that may be palpable on digital examination transrectal seminal vesiculotomy/vesiculectomy has also been recommended. Asymptomatic patients may be kept on observation and follow up. Currently, surgical extirpation of the SV rarely necessary though indicated chiefly as an adjunct to radical cystectomy, prostatectomy, and or urethrectomy or it may be needed for managing benign cysts and tumors of the SV. Recently, this has been accomplished laparoscopically, successfully in children and adults. An endoscopic approach is generally reserved only for associated stones involving the ejaculatory ducts.[2] We reported the present case as an interesting radiological image so as to alert and caution the attending urologist/surgeon to the possibility of SV calculi whenever such bean-shaped densities are seen laterally on a plane X-ray of the pelvis. This case also serves to heighten the awareness of the surgeon to the exclusion of vesical calculi thereby avoiding an inadvertent blunder of a fruitless cystolithotomy that has been reported elsewhere.[7] References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06009f1.jpg] [is06009t1.jpg] |
| |||||||||

{kind=link}
{kind=link}