 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
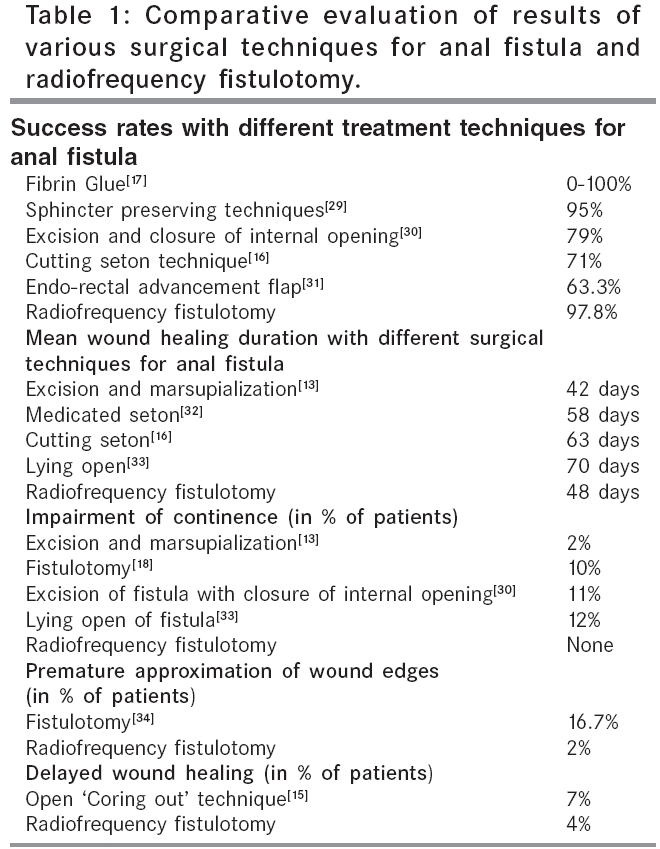
Indian Journal of Surgery, Vol. 68, No. 1, January-February, 2006, pp. 48-52 Point of technique Radio frequency fistulotomy: A better tool than the conventional techniques in anal fistula Gupta PJ Gupta Nursing Home, D/9, Laxminagar, Nagpur - 440 022 Code Number: is06013 Fistula in ano is defined as an abnormal communication, lined by granulation tissue between the anal canal and the exterior i.e. the skin, which causes a chronic inflammatory response. Most commonly, these fistulae develop following an anal abscess. Inadequate drainage of the abscess or a spontaneous rupture are the two main reasons for development of anal fistula. The occurrence of such abscesses is mostly secondary to infection of an anal gland [cryptoglandular hypothesis of Eisenhammer].[1] Tuberculosis, lymphogranuloma inguinale, inflammatory bowel disease like Crohn′s or ulcerative proctocolitis can also lead to development of anal fistula. Fistulae have been reported following external injury or probing an abscess or a low anal fistula.[2] A fistula may develop in a chronic anal fissure. A colloid carcinoma of the rectum can manifest itself through an anal fistula.[3] Other clinical conditions that can stimulate the appearance of a fistula include hidradenitis suppurativa, bilharziasis, actinomycosis and Bartholin′s gland abscess or sinus. According to Park, the anal fistula can be classified into four types- (i) Intersphincteric (ii) Transphincteric (iii). Supra sphincteric and (iv). Extra-sphincteric.[4] However, further variations of each can occur .[5] The classical lay open technique [Fistulotomy], is still the most favored procedure for the treatment of anal fistula.[6] Slitting the complete tract from the external to internal opening is the basis of the traditional fistulotomy. Tissues around the external and internal opening are excised along with a small margin of tissue lining the tract and the wound is kept open to allow healing by secondary intention.[7] The approach to conventional fistulotomy is as follows- While keeping the patient in a lithotomy position, digital palpation of the anal canal can delineate the tract as a nodule or a cord like structure, extending from the external opening to the anal canal. A hypertrophied anal papilla may be the point of internal opening, which can be located with an anoscope. Negotiating a director probe with a delicate hand either in a retrograde [preferred] or ante- grade course of the fistula, helps in transversing the tract. This is done with utmost gentleness to avoid creating a false passage. Instead, methylene blue or milk mixed with hydrogen peroxide is injected from the external opening, to locate the direction and path of the tract.[8] With the director probe inside the fistula, the track is cut along the probe. The edges of wounds are trimmed to remove about 1-3 mm of tissue margins. The wound is left open to heal from the base. The conventional fistulotomy is performed using a surgical knife and scissors, or electrocautry. We employed a radiofrequency device, Ellman Dual Frequency 4 MHz radiofrequency generator [Ellman International, Oceanside, N.Y.], to perform the functions of the conventional instruments. Radio frequency surgery is a technique of performing simultaneous cutting and coagulation of the tissues, using a high frequency alternate current. Such combined effect is produced by tissue resistive heating, from the passage of high frequency wave through them. This heat makes the intracellular water to boil and increases the cell inner pressure to the point of breaking it from inside to outside [explosion].[9] This phenomenon is called "cellular volatilization". As the intracellular tissue water provides the resistance and ultimately gets vaporized, it does not cause the heat and damage, as in the case of an electro cautry. The tissue vaporization also results in significant hemostasis, without actually burning the tissue. In addition, there is no danger of shocking or burning the patient for reason of controlled and minimal lateral tissue damage, with this device.[10] The radiofrequency unit is provided with a handle, to which different electrodes can be attached, as per the requirement of the procedure.[11] We used a ball electrode for coagulation, a needle electrode to incise the fistula tract and a round loop electrode to shave the surrounding infected tissue during our procedure. The aim of the present study is to explain this modified surgical technique, the postoperative events and the early and late complications that followed the procedure. There is also an attempt to compare the outcome of this procedure with the published data, on other approaches to treat low anal fistula. Patients and Methods Between July 1999 and June 2002, we operated 188 patients (137 males) with low anal fistula at our hospital, using a radio frequency device. The mean age of the patients was 37 yrs [range 22-63 yrs]. The mean duration of the disease was 19 months [range 4 months-11 yrs]. 17 patients with recurrence were also included in the study. Exclusion criteria: Only low fistulas with internal opening below the ano rectal ring were included for study. High trans- sphincteric fistulas with or without high blind tract, suprasphincteric, extrasphincteric and horseshoe fistulas, as well as fistulae associated with inflammatory bowel disease were excluded. Patients in whom the internal opening could not be located, were kept out of this study. Patients were operated under a short-term general anesthesia, or a caudal block at the discretion of the anesthesiologist. Informed consent was obtained from the patients. The trial was approved by the local ethics committee and was performed in line with the "Declaration of Helsinki". Recurrence was defined in the follow-up periods, as perirectal sepsis or discharge occurring either at the same location as the original fistula, or in a new perianal locale. Radio frequency fistulotomy procedure The steps of the procedure were the same as described above with the following modifications A small amount of methylene blue mixed with hydrogen peroxide was instilled from the external opening through an injection syringe. The emergence of the same from the internal opening was located by retracting the anal canal with anal speculum, or by inserting a slotted anoscope. A director probe was inserted in the tract from the external opening, to bring it out from the internal opening. The skin overlying the probe was coagulated by applying the ball electrode over its complete length. This reduced the amount of bleeding when the tract was slit open. The complete fistulous track was then cut open along the probe, with the help of the needle electrode. At times, there was a spurt of bleeding, which needed to be caught in a hemostat, which was then coagulated with the ball electrode. The wound edges along with the surrounding infected and fibrotic tissues were shaved with the loop electrode. As cutting and coagulation was achieved simultaneously, we could avoid the brisk bleeding often encountered in the conventional knife and scissor dissection. This shaving of the edges was fashioned in a manner that produced a pear shaped wound tapering towards the anus. This was done to prevent any premature approximation of the wound edges, during the course of healing of the underlying wound. A piece of the tract tissue was subjected for histopathological examination. Post operative care Patients were asked to take a 50 mg tablet of Diclofenac Sodium twice in a day for the first five postoperative days and then, as and when they felt pain. They were also prescribed a 400mg tablet of Ofloxacin, once a day, for ten days. No special wound care was advised, except a warm water sitz- bath twice in a day. An absorbent pad was used to cover the wound. The patients were examined in the evening of the procedure and were discharged if there were no complaints. They were called for follow-up every two weeks, until the wound healed. Frequent office visits during the postoperative period helped in educating the patient with appropriate wound care hints. Results In the present study, the patients were followed for a minimum of 2 years after the procedure. It took a mean time of 48 days for complete epithelization of the wound [range 32-95 days]. The average duration of incapacity for work was 5 days [range 3-13 days]. The mean analgesic requirement was 18 tablets of Diclofenac Sodium [range 14-31 tablets]. In 7 patients, delayed wound healing was observed, where the wounds took about 80-108 days for complete healing. Four patients had a premature closure of the proximal wound, while the distal end remained unhealed. In these patients, the healed edges of the proximal wound were slit opened with a needle electrode of the radiofrequency device, under local anesthesia. Three of such wounds healed uneventfully thereafter, while a small wound of the remaining patient,continued to discharge. This patient was labeled as a case of ′failure of wound healing′, rather than a case of recurrence. In two of the operated patients, the histopathological report suggested presence of tuberculosis. Antitubercular medication with a standard protocol was prescribed. Both of them had an uneventful recovery. None of the patients operated with this technique had any interference with continence. None developed anal stenosis or mucosal prolapse. At the last follow-up, 3 patients reported with recurrence of the fistula. Complications No major complications were encountered during or after radiofrequency fistulotomy. Few infrequent undesirable outcomes were noted in some initial cases. They included, an unusually long time taken for wound healing with excessive scarring,due to deep dissection. Few others reported with an edema around the wound, with excessive discharge from the open wound,because of excessive coagulation of the wound surface. With experience, we can successfully overcome these technical lacunae. Discussion A variety of treatment options have been reported for treatment of anal fistula. These include fistulectomy,[12] fistulotomy with marsupialization,[13] curettage of fistula and placement of flaps of mucosa or skin,[14] open coring out [sphincter preserving] technique,[15] placement of medicated setons,[16] insertion of antibiotic beads and injection of commercial or autologous fibrin glue.[17] In spite of availability of such options, a majority of the surgeons still rely on the classical lay open technique [fistulotomy], as the ′gold standard′for treatment of fistula- in-ano.[18] The patient satisfaction after surgical treatment for anal fistula, depends on factors like period of hospitalization, postoperative pain, return to routine activity, wound care and wound healing time, interference with the anal continence adversely affecting patient′s lifestyle and most importantly, the recurrence of the disease.[19] On all these fronts, the technique used by us, has been found to score over conventional fistulotomy, in the sense, that the time taken for the whole procedure is short, intra-operative bleeding is negligible and the use of suture material is altogether dispensed with. The period of hospitalization is less than a day, with work incapacity of less than a week. The wound healing is quick, without the need of any special wound care. While none of the patients in our study had any interference with the continence, the failure of wound healing/recurrence rate was as low as 2.2%. Radio frequency surgery may not be confused with electro surgery, diathermy, spark-gap circuitry, or electrocautry. Unlike electrocautry or diathermy, which works on the frequency between 0.5 to 1.5 MHz, radiofrequency uses a very high frequency current of 4 MHz. Unlike the electrocautry, the tip of the electrodes used in radiofrequency remains cold during its application.[20] This allows the surgeon to work in direct proximity of the functional tissues that need to be preserved.[21] As contrast to true cautry, which causes damage similar to 3rd degree burns, the tissue damage that does occur with radiofrequency is very superficial and is comparable to that which occurs with lasers. The radiofrequency device allows cutting and coagulation of tissues in an atraumatic manner, in contrast to the traditional electrosurgical devices. With radiofrequency, the targeted tissue temperatures stay localized within a 60-90° C range thus limiting heat dissipation and avoiding damage to adjacent healthy tissue. In juxtaposition, electrocautry, diathermy, or laser temperatures are significantly high (750-900° C) and result in significant heat propagation, far in excess of the therapeutic needs.[22] While techniques using conventional scalpel apparently work in an atraumatic way, the prominence of bleeding from the wound, invariably forces the surgeon to coagulate the bleeders more frequently. This results in excess tissue assault and the resultant complications. Histologically, it has been shown that tissue damage with radio frequency surgery is actually less, than that caused with a conventional scalpel and equals cold scalpel.[23] As radio frequency surgery creates minimal collateral heat damage in the tissue, wound healing is rapid and the scar is soft and supple.[24] It has been shown that the biopsies of the skin performed with radiofrequency, indicate that the maximum thickness of heat-denatured collagen is 75 micrometers. This equals, or is even better than that achieved with a carbon-dioxide laser.[25] Saving on treatment time, a nearly bloodless field, minimal postoperative pain and rapid healing are but a few advantages of radio frequency surgery.[26] Once the proper technique is established, a scar caused by this technique will be less pronounced, than that produced by other surgical techniques. Deeper excision increases the likelihood of scars.[27] The possible reasons for failure of fistulotomy wound to heal, or for recurrence of the disease are multiple. While premature union of the skin edges, failure to correctly excise the internal opening and failure to locate any extra tract are the prime causes, failure to detect a cavity leading upwards from the main tract, presence of foreign bodies and poor post fistulotomy wound care are few others to mention.[28] The results of radiofrequency fistulotomy are comparable, or even better than those with other approaches. [Table - 1] Conclusion It can be concluded that the radio frequency technique is cost effective as compared to the conventional one, due to reduction in hospital stay and reduced period off work. While it is agreeable that more controlled and randomized studies comparing this technique with other techniques of fistulotomy are needed, the initial results of this approach are doubtlessly encouraging[34].References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06013t1.jpg] |
| |||||||||

{kind=link}