 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
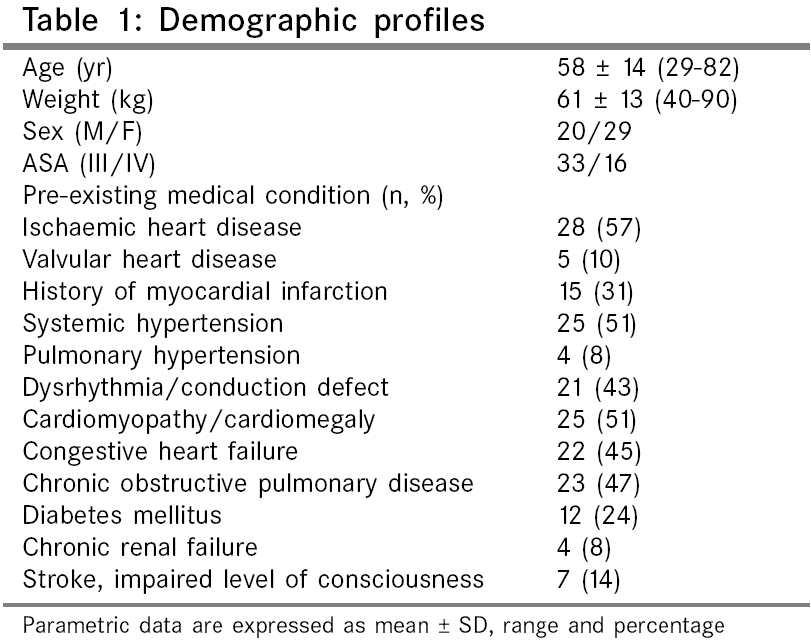
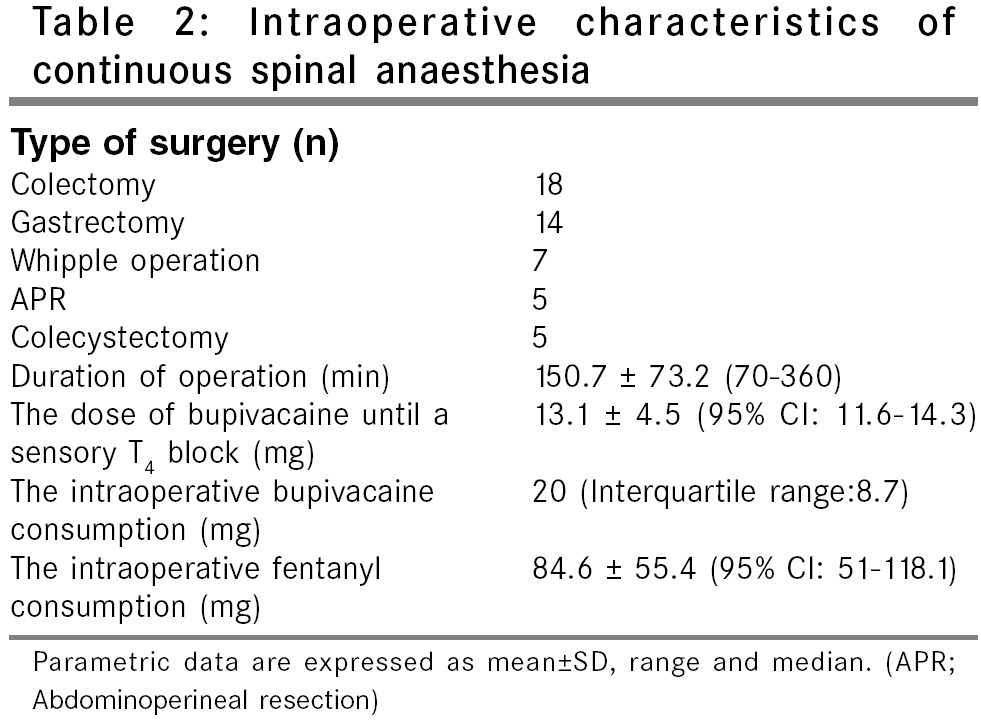
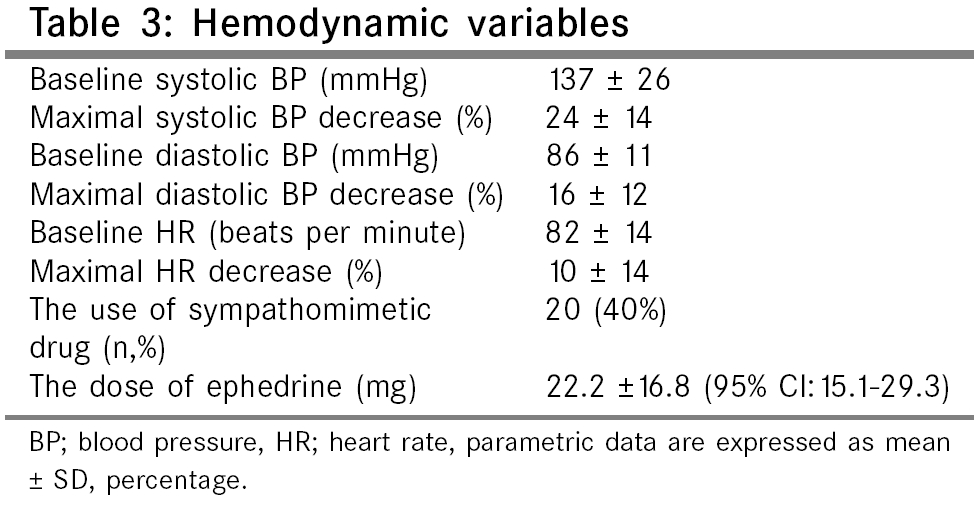
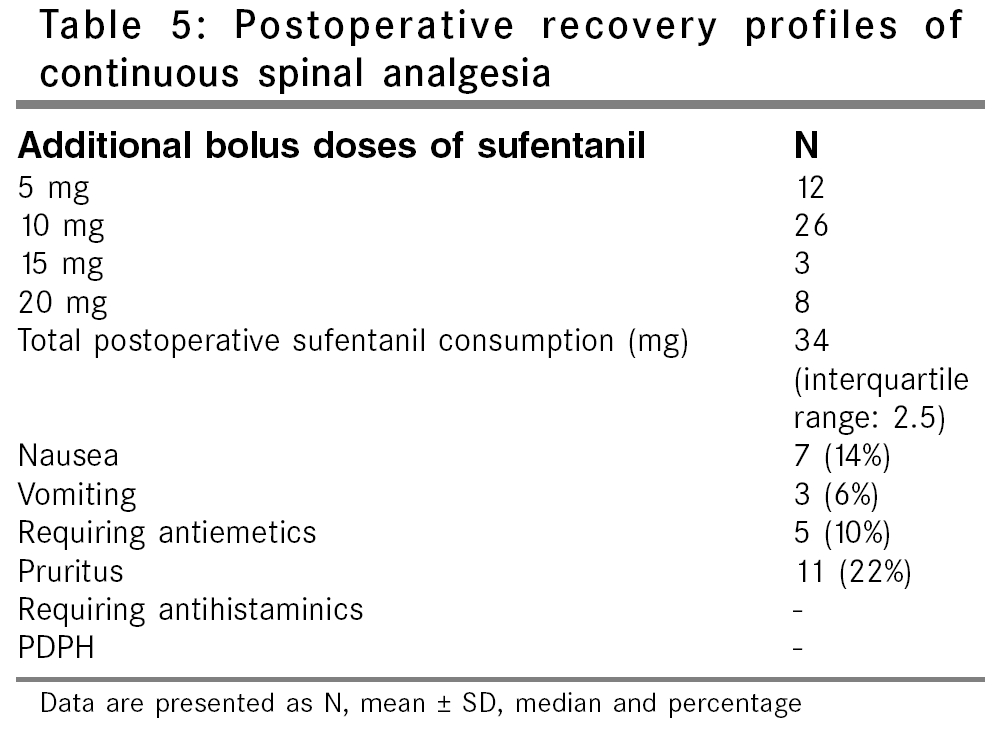
Indian Journal of Surgery, Vol. 68, No. 2, March-April, 2006, pp. 73-79 Original Article Continuous spinal anaesthesia and analgesia in high-risk patients undergoing abdominal surgery Gulcin Ö, Kaya Mensure, Gonca T, Özgur C, Saadet D, Serpil S, Nihal K Department of Anaesthesiology, Ankara Oncology Hospital, Ankara Code Number: is06020 Abstract Background: Continuous spinal anaesthesia has been used as a possibly safer technique than general anesthesia alone, in high-risk patients with a more predictable effect and lesser hemodynamic and respiratory repercussions.Aim: To evaluate the consequences of continuous spinal anaesthesia and analgesia, in 52 high-risk patients undergoing major abdominal surgery. Settings and Design: Operating room and postanaesthesia care unit of an oncology hospital; a prospective study. Materials and Methods: After inserting the 22 gauge spinal catheter, plain 0.5% Bupivacaine 7.5 mg was administered through the catheter. Additional doses of Bupivacaine 2.5 mg were given, until a sensory T 4 level and total dose was noted. The postoperative analgesia involved a continuous intrathecal infusion of Sufentanil 1 mg h -1 with Bupivacaine 1 mg h -1. Pain scores and side effects were assessed at 1, 2, 4, 6, 12, 18 and 24 h after the surgery. Results: The dose of Bupivacaine required to achieve the sensory T 4 level, was 13.1±4.5 mg. Forty percent of patients had hypotension and were easily controlled by the intermittent intravenous bolus of Ephedrine (22.2±16.8 mg). The technique provided effective analgesia with low dynamic and static pain scores and a low incidence of minor side effects such as nausea (14%), vomiting (6%) and pruritis (22%). Statistical Analysis: Kolmogorov Smirnov test was used to analyze the distribution of the data. Data are presented as mean ± SD, median, range or percentages. Conclusions: We concluded that continuous spinal anaesthesia and analgesia for the perioperative management could be performed effectively and safely, in high-risk patients with minimal adverse effects. Keywords: Anaesthetic technique, continuous spinal anaesthesia, analgesia, postoperative, patients, high-risk, humans. Continuous spinal anaesthesia (CSA) is a well-established technique, that has been used successfully in many surgical procedures.[1],[2] CSA has been acknowledged by many authors as a constituting safer technique in application to high risk patients, for it allows greater control over both induction and surgical anaesthesia, with a more predictable effect and lesser hemodynamic and respiratory repercussions, than both central neuraxial blockade and general anaesthetic techniques.[3],[4],[5] As the level of the block is established after patient positioning, hemodynamic and respiratory stability may be better preserved than single dose spinal anaesthesia. In addition, local anaesthetics or opioids alone, or in combination, may be administered intrathecally through a spinal catheter to provide postoperative analgesia.[6],[7] Nevertheless, there are only a few reports in the literature regarding the use of CSA in abdominal surgery requiring higher level of sensorial block. The present study was designed to evaluate the efficacy of continuous spinal anaesthesia in high-risk surgical patients undergoing major abdominal procedures. In addition, the safety and efficacy of continuous intrathecal infusion of Sufentanil combined with Bupivacaine for postoperative pain relief was investigated. Materials and Methods Fifty two patients scheduled for major abdominal surgery were enrolled in the study. Patients in class III-IV of Modified Goldman Cardiac Risk Index and/or ASA III-IV were accepted as at high risk. This prospective study was conducted after written informed consent of patients and approval from the hospital ethics committee. Exclusion criteria included patients with neurological deficits, coagulation disorders and obesity (BMI>30). If prophylactic low molecular weight Heparin (LMWH) would be utilized, it was given subcutaneously 2 h after insertion of the spinal catheter. In patients who were already receiving LMWH, the spinal catheters were inserted at least 12 hours after the last dosing. Patients were not premedicated. The day before surgery, each patient was taught the 10 cm visual analogue scale (VAS 0 = no pain, 10 = the worst possible pain). In the operating room, after recording baseline vital signs, each patient received 10 ml kg -1 of Ringer's lactate solution intravenously over 20-30 min, prior to the block. Spinal puncture was performed with the patient, in either sitting or in the lateral decubitus position, via the L 3 -L 4 or the L 4 -L 5 intervertebral space, using a midline approach under aseptic conditions. An 18 gauge Crawford-type epidural needle was used as an introducer and placed in the epidural space by loss of resistance technique. Then, a 22 gauge spinal catheter over a 27 gauge Quincke-type spinal needle was placed (Spinocath®, B. Braun, Melsungen, Germany). The catheter was inserted 3-4 cm into the subarachnoid space. Correct positioning of the catheter within the subarachnoid space was confirmed by the establishment of free cerebrospinal fluid (CSF) flow and a bacterial filter was attached. Procedure-related paresthesias, pain, or any difficulty during spinal puncture and catheterisation, were recorded in each case. With patients in the supine position, initial dose of plain 0.5% bupivacaine 7.5 mg (Marcaine® 0.5% Astra-Zeneca, UK) and sufentanil 10 mg (Sufenta® Janssen-Cilag, Belgium), were injected intrathecally. Bilateral dermatomal level of analgesia and the degree of motor block were assessed at 10 min after the initial dose of Bupivacaine. Additional bolus doses of Bupivacaine 2.5 mg were given every 5 min, until a sensory T 4 level was achieved, as defined by pinprick test along the midclavicular line and motor block was monitored using a modified Bromage scale (0 = no impairment of movement of leg and feet, 1 = inability to raise extended leg against gravity but able to flex knee, 2 = unable to flex knee but able to move feet, 3 = complete motor block). After bolus injection, the catheter was cleared by subsequent injection of 2 ml saline. Failure of the technique was considered to have occurred when surgical anaesthesia was not achieved after 45 min (maximum total dose of plain 0.5% bupivacaine up to 25 mg). Incremental bolus doses of Bupivacaine 2.5-5 mg were given during surgery, when the patient complained of pain or sensorial block regressed two segments. Patients were monitored continuously by invasive arterial blood pressure measurements, in addition to standard monitoring, consisting of electrocardiogram, heart rate, respiratory rate and pulse oximetry. All parameters were recorded at 5 min intervals during the surgery. The data recorded at 5 min intervals during the first 60 min and then every 15 min, until the end of the operation, was used for statistical analysis. We also closely followed arterial blood gases and acid-base balance, urinary output, blood loss and the sensory level of anaesthesia. During the operation, patients received nasal oxygen at a rate of 2 L/min and blood loss was replaced in case of a hemotocrit level less than 30%, by transfusion of erythrocytes. Hypotension was defined as a decrease in Systolic blood pressure of more than 15% of the basal pre-anaesthetic value and was treated by bolus doses of ephedrine 5-10 mg. Atropine was administered if a clinically important bradycardia developed (heart rate< 50 beats/min or heart rate< 55 beats/min with hypotension). To improve patient comfort during surgery, Propofol 1-3 mg kg -1 h -1 was given by infusion and bolus doses of Fentanyl 1-2 mg kg -1 were administered if needed. After completion of surgery, patients were transferred to the Postanaesthesia care unit (PACU). In the PACU, when patients complained of pain and had a VAS score>3 at rest, a loading dose of Sufentanil 5 mg and plain Bupivacaine 2.5 mg were injected intrathecally and the intrathecal catheter was connected to an elastomeric pump (Easypump® Braun, France), which was loaded with 60 ml solution, containing Bupivacaine 0.5 mg ml -1 (plain 0.5% Bupivacaine 6ml) and Sufentanil 0.5 mg ml -1 (Sufentanil 6 ml) added to 48 ml NaCl 0.9%. The intrathecal infusion rate of 2 ml h -1 was maintained for 24 h. In case of recurrent pain greater than 3 on the VAS at rest, patients received additional bolus doses of 5 mg Sufentanil at 30 min intervals. Static and dynamic pain scores were assessed 1, 2, 4, 6, 12, 18 and 24 h postoperatively. Arterial blood pressure and heart rate were recorded every one-hour during the first postoperative 24 hr. All patients received 2 L min -1 oxygen via a nasal cannula and oxygen saturation was monitored continuously after surgery. The sedation score (1 = awake and alert, 2 = sedated, responds to verbal stimulus, 3 = sedated, responds to mild physical stimulus, 4 = sedated, responds to moderate or strong physical stimulus, 5 = not arousable) and respiratory rate were determined hourly, for 24 h. Respiratory depression was defined as a respiratory rate< 10 breaths min -1, or oxygen saturation< 95%, by pulse oximetry. The presence and severity of nausea and vomiting were especially asked and assessed by a nausea score; 0 = no nausea, 1 = mild nausea but no vomiting, 2 = nausea, easily relieved by vomiting and requiring no treatment, 3 = intractable vomiting requiring treatment. Metoclopramide 10 mg was given for intractable vomiting, by intravenous bolus on patient requests. Presence of pruritus was also questioned by the observer and medication to control severe pruritus (diphenhydramine 25 mg intravenous) was noted. Urinary retention was not assessed, because all patients had indwelling urinary catheters. At the end of 24 h, all patients were interviewed by an observer to evaluate their overall satisfaction in postoperative analgesic regimen, graded as, excellent, good, fair, or poor. The intrathecal catheters remained in situ for 24 hr. They were removed with patient lying on his side and in a flexed position, 12 h after the last dose of prophylactic Heparin if administered. All patients were visited daily during the first 10 postoperative days to assess any nerve root injury (radiculopathy, back pain, cauda equina), central nervous system complication (menengitis, spinal abscess, spinal hematoma) and post dural puncture headache (PDPH). Statistical analysis Statistical analysis was performed with SPSS statistical software (version 10.0; SPSS, Chicago, IL, USA). Data are presented as mean ± SD, median, range or percentages. Kolmogorov Smirnov test was used to analyze the distribution of the data. Results All anaesthetic and surgical procedures were completed without any major complication. One patient was given general anaesthesia, as the necessary segmental sensorial level was not obtained and two patients received analgesics, not according to the protocol. Two patients who received intravenous Meperidine 25 mg, for treatment of postoperative shivering on arrival in the PACU, were not excluded. The demographic characteristics, ASA classification, type and duration of surgery are presented in [Table - 1][Table - 2]. The catheters were placed in a sitting position in 71% of patients. Although dura was punctured inadvertently with an epidural needle in one patient, there was no difficulty in placing the catheter. In three patients, we had difficulty in withdrawal of the stylet of the catheter, but the catheter was easily placed in the subarachnoid space. Ten patients had transient paresthesia, or pain while threading the needle or/and the catheter. None of these patients developed neurological problems in the postoperative period. The mean Bupivacaine requirements for a sensory block at T 4 and doses of Bupivacaine used during the operation are shown in [Table - 2]. During surgery, a decrease in the Systolic blood pressure by more than 15% of the preanaesthetic baseline level, was noted in 20 patients (40%). Hemodynamic variables and the use of sympathomimetic drugs are presented in [Table - 3]. There were no respiratory or cardiovascular complications and all patients were discharged from the PACU . Respiratory depression as defined, was not observed. Postoperatively no patient needed vasopressors. The mean static and dynamic VAS scores, postoperative Sufentanil consumption and the need for additional bolus doses of Sufentanil are shown in [Table - 4][Table - 5]. At the end of surgery, 12 patients had complete motor block (Bromage scale point 3), 13 patients had scale point 2 and five patients had scale point 1. However, all patients were mobile in bed, 6 h postoperatively, with no residual motor block. Some degree of sedation was experienced by all patients and the sedation scores varied between 1 and 2 points for the first 24 h, postoperatively. All patients responded immediately when called and all were cooperative during physical exercise and were able to take deep breaths, cough and mobilize without discomfort. Seven patients had mild nausea and three had vomiting. Eleven patients complained of mild pruritus, which was not spontaneously reported and needed no treatment. Urinary retention was not detected, because all patients had indwelling urinary catheters. The degree of patients′ satisfaction of the technique of anaesthesia and analgesia, was found to be 56% excellent, 35% good and 9% fair. The spinal catheters were removed without any problem. PDPH and neurological deficits were not seen in any patient. There were no complaints of the back pain. Discussion This study describes the use of CSA technique during the perioperative period in high-risk patients undergoing major abdominal surgery and it proved to provide safe intraoperative anaesthesia and effective postoperative analgesia, with minimal side effects in the study population. With general anaesthesia, sympathetic stimulation and elevated levels of serum catecholamines during laringoscopy and intubation and after surgical incision, may increase the incidences of morbidity and mortality, especially in patients with cardiac risks.[8],[9] General anaesthesia also increases the intraoperative and postoperative complications in patients with chronic obstructive pulmonary disease.[10] Neuraxial or peripheral nerve blockade techniques are successfully applied, when there is a risk for general anaesthesia. However, regional anaesthesia during abdominal surgery is less preferred, because of several reasons such as, hemodynamic instability due to higher sensorial / sympathetic block, insufficient muscle relaxation, anxiety and physical discomfort for the patient, pain, vomiting and bradycardia due to peritoneal traction and insufficient clinical experience. Although absence of a control group is a deficiency of this study, patient satisfaction was obtained at a high rate and most of the disadvantages were successfully managed. The reason for the high incidence of hypotension in this study may be our criteria, defining hypotension as a decrease in the Systolic blood pressure by more than 15% of the preanaesthetic baseline level. Although hypotension occurred in 40% of patients and despite the T 4 sensory level of anaesthesia, the maximal Systolic blood pressure decrease was only 24%. We noticed small decreases in blood pressure from preoperative baseline values, which were easily controlled by the intermittent bolus of Ephedrine and the appropriate transfusion of fluids or blood. In our hospital, most of the surgeries are oncologic and the patients are generally anemic and dehydrated because of several reasons. We administered 10 ml kg -1 of Ringer′s lactate solution intravenously over 20-30 min, prior to the block, to prevent hypotension due to sympathetic blockade.[11],[12] When the hemotocrit level was less than 30%, blood transfusion was given in order to prevent an impairment of the oxygen carrying capacity. Packed red blood cells were used to avoid volume overload. The relative hemodynamic stability of CSA is probably due to the slow development of sympathetic blockade. It has been pointed out that the maximum hemodynamic effects produced by local anaesthetic injection may not occur for up to 20 min after CSA, thus giving time for the compensating mechanisms to develop.[13] Discomfort and pain during peritoneal traction were easily managed by Propofol infusion and additional Fentanyl boluses. This study shows that good analgesia can be obtained with a low-dose intrathecal infusion of Sufentanil 1 mg h -1 combined with Bupivacaine 1 mg h -1sub, after major abdominal surgery. Sufentanil is well suited for use via continuous intrathecal infusion, for postoperative analgesia. Its rapid ons et al lows easy titration to individual patient tolerance and the desired clinical endpoint. Its short duration of action means that the opioid′s desired analgesic effect will continue as long as the infusion is running; likewise, any undesirable side effects will be short-lived with discontinuation of the infusion. Only a limited number of reports documented the use of an infusion of intrathecal Sufentanil given for postoperative analgesia.[14],[15] Intrathecal Sufentanil has been used as a single injection drug and via continuous infusion for labor analgesia.[16] After major lower limb surgery, a single dose of Sufentanil 7.5 mg has provided complete postoperative pain relief lasting for 4 h.[17] Borgdoff et al have demonstrated that large-dose intrathecal Sufentanil (150 μg) prevents hormonal stress response during major abdominal surgery.[18] The doses used in the present study were chosen based on the previous reports in different surgery and patient groups. The use of intrathecal opioid, especially in higher doses, is associated with adverse effects such as respiratory depression, urinary retention, pruritus, nausea and vomiting.[19] There are no recommendations in the literature regarding analgesically efficacious intrathecal infusing doses of Sufentanil. In our study, the combination of intrathecal infusion of Sufentanil with Bupivacaine, thus using the low-doses of each drug, increased the efficiency of analgesia, without significant side effects. Lipid-soluble opioids are more suitable for intrathecal use. The early respiratory depression reported after intrathecal or epidural Fentanyl or Sufentanil, may develop rapidly within minutes to 2 h.[20] The respiratory depression has been reported in parturients[21] and after a single 5 mg bolus, in an elderly surgical patient.[22] Slow intrathecal continuous infusion of lipid-soluble opioids in small doses has the advantage over single larger dose in preventing high peak concentrations of the drug in the CSF, the incidence of respiratory depression thus being lower. In this study, the patients were admitted to a PACU for the duration of the infusion and were monitored with pulse oximetry and hourly respiratory rate checks. We used small doses and avoided the concomitant administration of sedatives and other opioid analgesics. None of our patients developed respiratory depression; nasal oxygen therapy and low grade of sedation reduced the likelihood of the undesirable side effects of opioids. Previous reports indicate that respiratory depression from intrathecal Sufentanil is preceded by somnolence and desaturation can be avoided with nasal oxygen therapy.[21] In our study, the incidence of pruritus for intrathecal Sufentanil was 22%, which is lower than that reported for laboring patients.[23],[24] In all our patients, pruritus was of mild intensity, not requiring treatment. The effective analgesia was associated with lower incidence of nausea and vomiting in this study. Some anaesthetists prefer intrathecal catheters to be removed as soon as possible after surgery, because of risk of infection or catheter breakage.[7],[14] In the present study, the catheters were also removed after 24 hr. Neurologic complications and particularly the cauda equina syndrome have been described with the use of CSA.[25] Their most likely cause is maldistrubition of the local anaesthetic, following a slow injection through a small end-hole catheter. Hyperbaric solutions of local anaesthetics are not preferred in CSA and especially not hyperbaric Lidocaine.[26] Van Gessel et al have found that the highest block levels were reached with hyperbaric solutions and more circulatory changes that needed treatment were experienced by these patients.[27] In the present study, we avoided using hyperbaric Bupivacaine or Lidocaine or hypobaric Bupivacaine. Although the reported neurological problems after CSA may be related to the small diameter of microcatheters, or to a high local anaesthetic dose or concentration,[25] such a complication occurred even after CSA was performed with macrocatheters.[28] Paresthesia during needle or catheter placement seems to occur in about 25%, but there does not seem to be a clear causal relationship between paresthesias and neurologic sequelae of the trauma.[29] In our study, none of the patients with paresthesias during the procedure were associated with neurologic deficits. One of the main reasons for the reduced gauge of the catheter and the introducer needle, was to diminish the incidence of PDPH and thus to extend application of the method to all patient groups. The results of our study show an incidence of PDPH in accordance with the< 1% reported in other studies.[30],[31] The use of the 22 gauge catheter over 27 gauge needle as in the present study, may offer an advantage by minimizing the problems derived from smaller diameter catheters. In the catheter over needle system, the catheter immediately seals the puncture hole, avoids CSF leakage and reduces the duration and intensity of PDPH.[32] The catheters smaller than 27 gauge are generally regarded as microcatheters. In the present study, we used a 22 gauge spinal catheter over a 27 gauge Quincke-type spinal needle. Conclusion In conclusion, given the need for larger studies with control groups, the results of this study suggest, that CSA can be performed effectively and safely in high-risk patients undergoing major abdominal surgery. We have demonstrated that the combination of a low dose of Sufentanil and Bupivacaine via intrathecal infusion produced good postoperative analgesia with minimal side effects. References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06020t4.jpg] [is06020t3.jpg] [is06020t1.jpg] [is06020t5.jpg] [is06020t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}