 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
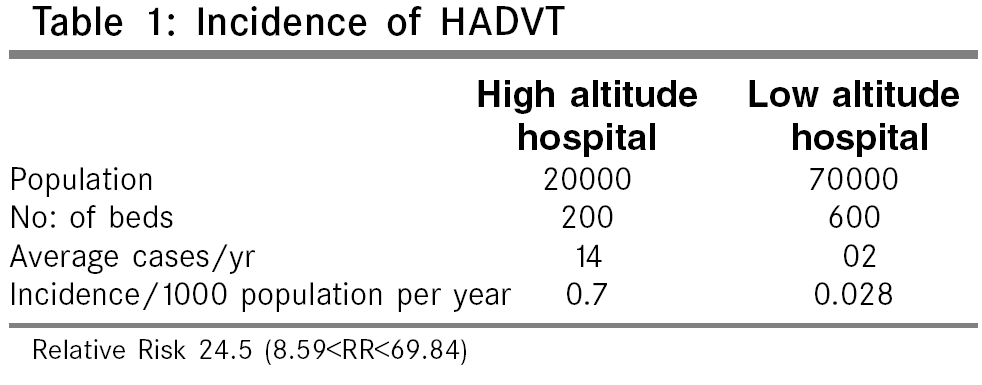
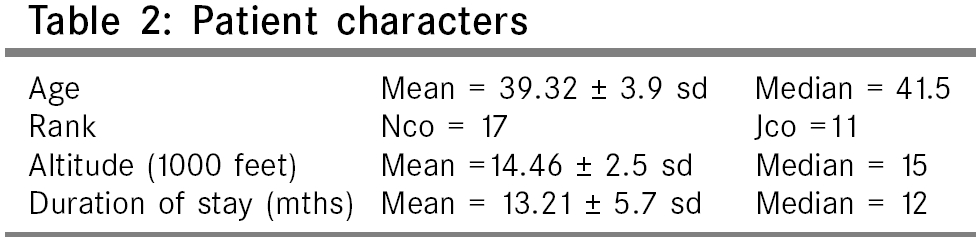
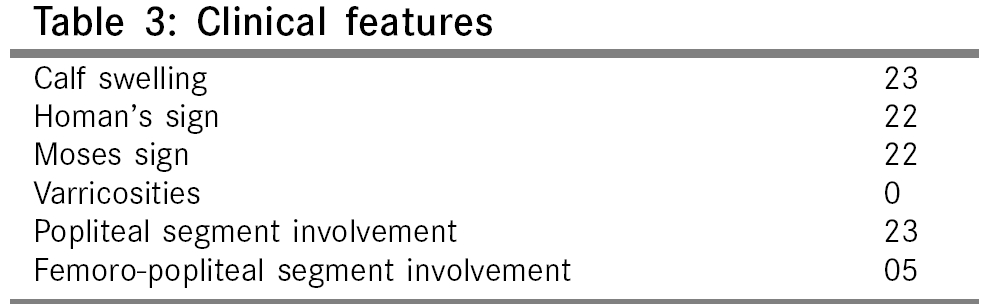
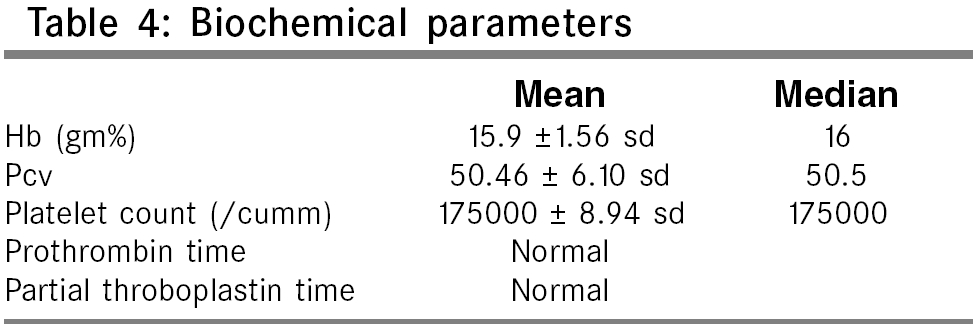
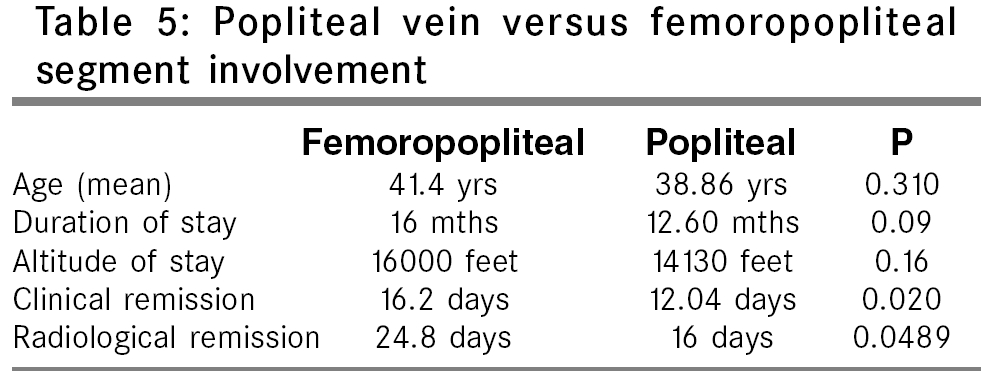
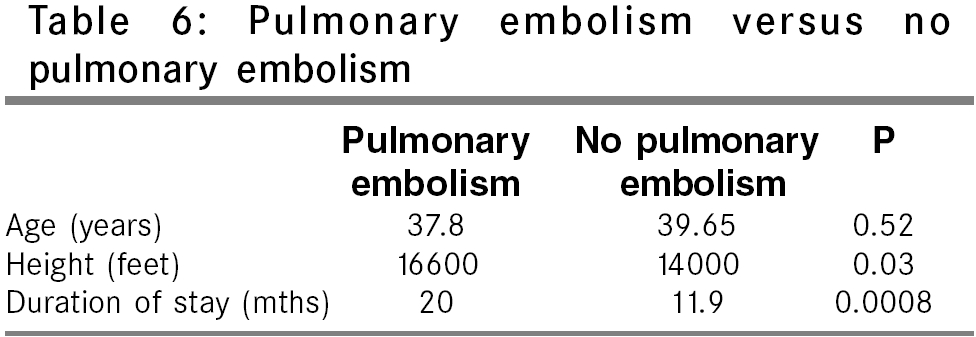
Indian Journal of Surgery, Vol. 68, No. 2, March-April, 2006, pp. 84-88 Original Article High altitude induced deep venous thrombosis: A study of 28 cases Kumar Shishir Department of Surgery, Military Hospital, Ambala cantt, haryana - 33001 Code Number: is06022 Abstract Background: It is well recognized that a hypercoagulable state exists when a person is exposed to high altitude environment. This may manifest as early thromboembolic episodes, which result in acute pulmonary embolism. On further exposure to high-altitude environment, the ongoing thrombogenesis has been implicated in the causation of subacute mountain sickness. Only anecdotal reports of deep vein thrombosis (DVT) of leg veins at high altitude exist in literature and only two studies of this disease entity have been reported in literature.Aim: To report the high incidence of deep venous thrombosis of leg veins at high altitude, as compared to lowlands and define the disease entity High Altitude Induced Deep Venous Thrombosis (HADVT). Setting and Design: Twenty-eight cases of deep venous thrombosis of leg veins occurring in Indian soldiers presenting to a high altitude hospital at 11,800 feet, staying in HA for a prolonged period of time (>5 months), were studied. The incidence of patients presenting to this hospital was compared with the incidence of deep venous thrombosis in a hospital situated in the lowland. Results: The annual incidence of deep vein thrombosis in lowlanders exposed to high altitude was much higher (0.7/1000) than in soldiers staying in lowland (0.028/1000). The relative risk of deep vein thrombosis was much higher among soldiers at high altitude as compared to soldiers in the plains. Long-term stay of lowlanders at high altitude was associated with a 24.5 (95% Confidence limits 8.59 to 69.84) times risk of deep venous thrombosis of the calf veins as compared to those staying in low altitude. Conclusion: In view of the greatly increased risk of getting deep venous thrombosis in leg veins at high altitude, we wish to define this definite disease entity as High Altitude Induced Deep Venous Thrombosis (HADVT). Keywords: Deep vein thrombosis (DVT), high altitude (HA), high altitude induced deep venous thrombosis (HADVT). High Altitude (HA) is defined as heights above 2,700 m (9,000 feet). Extreme High Altitude is defined as heights above 5,500-5,800 m (18,000-19000 feet). High Altitude, with its attendant hypobaric and cold conditions, results in certain stresses to the human body. To overcome these adverse effects of the environment, certain physiological changes occur, which if successful, lead to acclimatization of the individual. Failure, on the other hand, leads to the various maladies of high altitude. Apart from hypoxia and cold, other factors at high altitude that could affect performance and lead or contribute to illness include low humidity, solar and ultraviolet radiation. An important effect of high altitude is on the coagulation cascade in the body. On induction to high altitude, there is an initial hypercoagulable state, which persists for a few weeks but then slowly regresses as the patient acclimatizes due to a transient increase in clotting factors and platelet dysfunction.[1],[2],[3],[4] This is manifested clinically by Acute Pulmonary Thrombosis in lowlanders rapidly ascending to high altitude (mountaineers and trekkers).[5],[6] A few reports of DVT and cerebral, retinal and portal and splenic vessel thrombosis[7],[8],[9] have also been reported. This abnormality in clotting factors regresses after a few weeks, but on prolonged stay at high altitude (>5 months), there develops a hyperfibrinogenic state[9],[5] and persists for as long as the patient stays at high altitude. Clinically, late hypercoagulability has been demonstrated by Singh[10] in Indian soldiers who stayed in HAA for a period of 5-24 months and presented as pulmonary hypertension. Anand et al.[11] reported 10 cases of portal system thrombosis in Indian soldiers staying at high altitude for a mean duration of 12.4 months. There have only been two studies demonstrating DVT of leg veins in persons staying at high altitude for a prolonged period of time (>5 months).[12],[13] Materials and Methods This prospective study was carried out in a high-altitude hospital of the Indian Army located at a height of 11,800 feet. This hospital provided medical facilities to 20,000 lowlander troops located at a height of 10,000-20,000 feet in the Northern Sector. Twenty-eight patients of deep venous thrombosis of leg veins who were received in this hospital over a 2-year period formed the materials for the study. All these patients, apart from clinical examination, had color Doppler and venographic studies performed on them to document the presence of deep venous thrombosis. Baseline biochemical investigations in the form of Hb%, PCV, TLC, DLC, prothrombin time, partial thromboplastin time with kaolin, platelet count, ECG and x-ray chest were done on these patients. Deep venous thrombosis was defined on the clinical criterion of limb edema with or without limb tenderness and demonstration of thrombosis on color Doppler and venography and the absence of flow in the deep veins. Nonfatal pulmonary embolism was defined clinically when a patient had associated breathlessness; cough with or without hemoptysis; deranged paO2; a right ventricular strain pattern on ECG, with or without radiographic evidence of pulmonary infarction; and when high altitude pulmonary edema (HAPO) was ruled out. On confirming the presence of deep venous thrombosis in the leg veins, these patients were started on an immediate infusion of Inj. Heparin 1000 units per hour and the dosage titrated subsequently as per partial thromboplastin time with kaolin, which was done daily. 48 h after the heparin therapy, these patients were started on Acitrome 4 mg OD and therapy again titrated as per prothrombin time. Daily color Doppler studies were performed to document the flow through these veins and when flow was seen through these veins, the flow was documented by a repeat venograph. The clinical response to the therapy was noted by decrease in pain, calf tenderness and calf swelling; and radiological evidence of recanalisation of leg veins was obtained by color Doppler and venogram. These patients were evacuated from high altitude and were continued on oral anticoagulants, which were stopped after 3 months. Data was also collected for the corresponding period from a lowland hospital located in Northern India having 600 beds and catering to a population of 70,000. The number of cases of deep venous thrombosis of the leg veins received in this hospital was recorded. The incidence of DVT in soldiers staying at high altitude was compared with the incidence of DVT from the low-altitude hospital and statistically analyzed using EPI - Info 2002 software. Observations Twenty-eight patients of deep venous thrombosis of leg veins were received in the high-altitude hospital. This high-altitude hospital was catering to a population of 20,000 lowlanders, making the incidence of HADVT as 0.7/1000 population. We compared this to the incidence of a 600-bedded zonal hospital in peace area in plains of northern India, which had an average of only two cases of DVT per year and catered to a population of 70,000. None of these patients had any known risk factors of DVT (incidence=0.028/1000 population). Soldiers at high altitude had a relative risk of 24.5 as compared to soldiers in the plains for deep vein thrombosis (95% confidence limits 8.59< RR< 69.84). All patients received were males. Twenty-two out of the 28 patients (78.57%) patients had florid clinical signs of deep venous thrombosis in the form of positive Homan′s and Moses′sign and calf edema. The mean Hb% of these patients was 15.9 gm% (median=16 gm%). The other biochemical parameters of these patients were within normal limits. Twenty-seven of the 28 patients survived. One patient of massive pulmonary embolism died and necropsy showed a large embolus straddling both the pulmonary vessels and extending to the right atrium. The mean time to clinical response was 12.78 days (media = 13 days). The mean time to radiological clearance was 17.5 days (median =16.5 days). Twenty-three (82.14%) had involvement of only the popliteal vein, while 5 (21.42%) patients had involvement of the femoropopliteal segment. There was no statistically significant difference in these groups as far as their age, duration of stay and the height of stay was concerned. Both clinical and radiological remission in patients with femoropopliteal segment as compared to those of only popliteal segment involvement was significantly delayed. There were six patients who had associated evidence of pulmonary embolism. On comparison of these patients, we observed that pulmonary embolism occurred in patients who were staying at a higher altitude and for longer duration as compared to those who did not have pulmonary embolism. This relationship, though statistically significant, is limited due to the lesser number of patients in the study. The results are summarized in [Table - 1][Table - 2][Table - 3][Table - 4][Table - 5][Table - 6]. Discussion Hypercoagulable states in individuals exposed to high altitude and suffering from acute pulmonary edema, subacute mountain sickness and chronic mountain sickness has been demonstrated. However, unequivocal changes in blood coagulation have neither been demonstrated nor defined. According to Chohan et al,[1] there is an immediate hypercoagulability on arrival at high altitude, as evidenced by increase in platelet count, heightened levels of factor X and XII, shortening or prothrombin time and impairment of clot retraction. There was a compensatory rise in fibrinolytic activity, as gauged by the reduction of clot lysis time of plasma fibrinogen.[9] This rise in hypercoagulability shows a peak by the end of the first week and then slowly starts to abate by the end of the second week when the hematocrit rises. There is a decrease in the levels of the clotting factors and the reversal of prothrombin, clot retraction and clot lysis time to normal. As the individual continues to stay at high altitude, there is an increase in plasma fibrin activity,[10] thereby leading to a persistent hypercoagulable state and which reaches peak beyond 5 months of stay and continues till the individual stays at high altitude. Despite the conflicting views on early hypercoagulability, it is certain that thrombotic episodes do occur early on rapid exposure to high altitude and may take the form of pulmonary thrombosis, splenic, mesentric, cerebral or peripheral thrombosis.[7],[8],[14] Ward[6] reported three cases of DVT of calf veins in climbers who ascended to extreme high altitude (5,790-7,930 m). Genton et al reported a similar case in patients climbing to Mt Goodwin Austin.[5] Dickinson and Heath[7] reported seven cases of deaths in unacclaimatised trekkers in Himalayas at heights above 5,000 feet. Five of these patients had pulmonary thromboembolism, but only one person had demonstrable HADVT of calve veins. A similar case of deep venous thrombosis in calve veins has been reported by Virginia Robinson in the Canadian Everest expedition 2000.[15] Thrombotic episodes on prolonged stay at high altitude have been reported by Singh and Chohan[9] who demonstrated thrombotic occlusive hypertensive vascular disease in Indian soldiers residing at high altitude for duration of 5 to 24 months. They also showed three cases of deep venous thrombosis of the calf veins apart from thrombosis of cerebral, coronary and mesenteric arteries. Similar chronic thrombosis of pulmonary vessels has been demonstrated by Presti et al[16] who found the incidence of chronic massive thrombosis of pulmonary artery to be 0.9%. Recently Anand et al have also demonstrated systemic venous thrombosis in soldiers staying at extreme high altitude for prolonged periods of time.[14] Anand et al. demonstrated 20 cases of DVT of calf veins in Indian soldiers residing above 5,000 m for more than 10 months.[12] Similar DVT of calf veins was demonstrated in Pakistani soldiers staying at high altitude for a prolonged period of time.[13] Thus very few reports of deep venous thrombosis of leg veins on prolonged exposure to high altitude exist. We are documenting 28 such patients seen in a 2-year period and are defining this disease entity as High Altitude Induced Deep Venous Thrombosis (HADVT). The incidence of this disease in our population group is 0.7/1000 and significantly higher than the incidence of deep venous thrombosis in plains (0.0285/1000). The relative risk of getting DVT for a soldier at high altitude was 24.5 times higher as compared to soldiers in the plains (95% confidence limits 8.59< RR< 69.84). In the 28 patients of HADVT that we saw, the mean age was 39.2 years (range 32-40). Majority of patients (64.2%) were greater than 40 years of age. These patients were generally an older lot of patients as compared to the average age of Indian soldiers on that altitude (27 years). This is likely to be due to the fact that the older lot of soldiers did less exercise compared to their younger counterparts, thereby exposing them to greater stasis in the peripheral veins. The mean altitude at which these individuals stayed was 14,464 feet (range 10,000-18000 feet). Most of the soldiers who suffered from HADVT were from regions at a height of 12,000-16,000 feet, which is moderately high altitude. This contrasts with the studies of Ward,[17] Genton[5] and Anand[12] that deep venous thrombosis and pulmonary thrombosis occurred only at extremely high altitudes and correlates well with the studies of Presti et al,[15] who reported chronic thrombosis of pulmonary vessels at moderate altitude. Thus it is clear from our study that there is ongoing thrombogenesis even at moderate altitude and it is not confined to very high altitude alone. The mean duration of stay at the altitude was 13.21 months (range 5-24 months). From this figure, one can see that a large number of HADVT occurred in the first 10 months (39.28%), whereas 21.4% were affected in the period between 10 and 14 months and 25% between 14 and 18 months. Since no case of HADVT occurred before 5 months of stay at high altitude, it can be safely deduced that there is an ongoing thrombogenesis on prolonged stay at high altitude leading to HADVT. As we′ve seen from [Table - 5], there is an early clinical and radiological restoration of flow in popliteal vein as compared to femoropopliteal segments and this was found to be statistically significant, though the sample size is small. From [Table - 6] it can be seen that the acute pulmonary embolism is significantly higher in individuals who stayed at higher altitude and for prolonged periods of time. This needs to be evaluated by further studies. The biochemical evaluation of patients revealed average hemoglobin of 15.5 g/dl and an average PCV of 50.5. There was no derangement of bleeding time, clotting time, prothrombin time or partial thromboplastin time with kaolin. There was also no change in platelet count. Since all our patients had stayed at HAA for prolonged periods of time, it is possible that the hypercoagulability was due to hyperfibrinogenemia. However, we had no facilities for measuring fibrinogen levels and this needs to be investigated further. Conclusion Only a few cases of deep venous thrombosis of the leg veins in patients staying at moderately high altitude for prolonged periods of time have been reported in literature. A disease entity called High Altitude Induced Deep Venous Thrombosis (HADVT) exists, which is likely to occur in lowlanders staying at moderately high altitude for prolonged periods of time. The basic hematological work-up in these patients does not reveal any clotting abnormality. These individuals are likely to have either a popliteal vein or a femoropopliteal block and the femoral vein is likely to recanalize later than the popliteal vein. Also, many of these patients may present with acute fatal or nonfatal pulmonary embolism and this is likely to occur in those who stay at moderately high and extremely high altitude for very long periods. The cause of the hypercoagulable state in the patients of HADVT needs to be further studied by more sophisticated biochemical methods.References
Copyright 2006 - Indian Journal of Surgery The following images related to this document are available:Photo images[is06022t4.jpg] [is06022t3.jpg] [is06022t1.jpg] [is06022t5.jpg] [is06022t6.jpg] [is06022t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}